
Page 264 - Textbook of Pathology, 6th Edition
P. 264
248
ii) Squamous metaplasia of pancreatic ductal epithelium may
lead to obstruction and cystic dilatation.
iii) Squamous metaplasia of urothelium of the pelvis of kid-
ney may predispose to pyelonephritis and perhaps to
renal calculi.
iv) Long-standing metaplasia may cause progression to
anaplasia under certain circumstances.
v) Bone growth in vitamin A deficient animals is retarded.
vi) Immune dysfunction may occur due to damaged barrier
SECTION I
epithelium and compromised immune defenses.
vii) Pregnant women may have increased risk of maternal
infection, mortality and impaired embryonic develop-
ment.
HYPERVITAMINOSIS A. Very large doses of vitamin A
can produce toxic manifestations in children as well as in
adults. These may be acute or chronic.
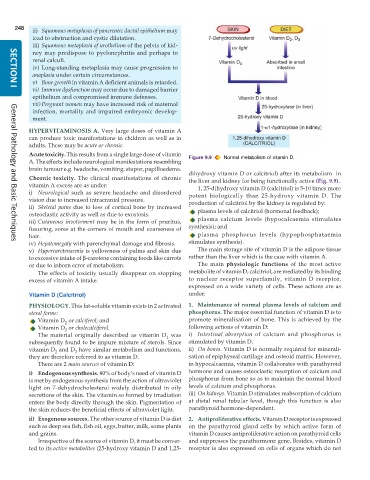
Acute toxicity. This results from a single large dose of vitamin Figure 9.9 Normal metabolism of vitamin D.
A. The effects include neurological manifestations resembling
brain tumour e.g. headache, vomiting, stupor, papilloedema.
dihydroxy vitamin D or calcitriol) after its metabolism in
Chronic toxicity. The clinical manifestations of chronic the liver and kidney for being functionally active (Fig. 9.9).
vitamin A excess are as under: 1, 25-dihydroxy vitamin D (calcitriol) is 5-10 times more
i) Neurological such as severe headache and disordered potent biologically than 25-hydroxy vitamin D. The
vision due to increased intracranial pressure. production of calcitriol by the kidney is regulated by:
ii) Skeletal pains due to loss of cortical bone by increased plasma levels of calcitriol (hormonal feedback);
osteoclastic activity as well as due to exostosis.
iii) Cutaneous involvement may be in the form of pruritus, plasma calcium levels (hypocalcaemia stimulates
fissuring, sores at the corners of mouth and coarseness of synthesis); and
hair. plasma phosphorus levels (hypophosphataemia
iv) Hepatomegaly with parenchymal damage and fibrosis. stimulates synthesis).
General Pathology and Basic Techniques
v) Hypercarotenaemia is yellowness of palms and skin due The main storage site of vitamin D is the adipose tissue
to excessive intake of β-carotene containing foods like carrots rather than the liver which is the case with vitamin A.
or due to inborn error of metabolism. The main physiologic functions of the most active
The effects of toxicity usually disappear on stopping metabolite of vitamin D, calcitriol, are mediated by its binding
excess of vitamin A intake. to nuclear receptor superfamily, vitamin D receptor,
expressed on a wide variety of cells. These actions are as
Vitamin D (Calcitriol) under:
PHYSIOLOGY. This fat-soluble vitamin exists in 2 activated 1. Maintenance of normal plasma levels of calcium and
sterol forms: phosphorus. The major essential function of vitamin D is to
Vitamin D or calciferol; and promote mineralisation of bone. This is achieved by the
2
Vitamin D or cholecalciferol. following actions of vitamin D:
3
The material originally described as vitamin D was i) Intestinal absorption of calcium and phosphorus is
1
subsequently found to be impure mixture of sterols. Since stimulated by vitamin D.
vitamin D and D have similar metabolism and functions, ii) On bones. Vitamin D is normally required for minerali-
2
3
they are therefore referred to as vitamin D. sation of epiphyseal cartilage and osteoid matrix. However,
There are 2 main sources of vitamin D: in hypocalcaemia, vitamin D collaborates with parathyroid
i) Endogenous synthesis. 80% of body’s need of vitamin D hormone and causes osteoclastic resorption of calcium and
is met by endogenous synthesis from the action of ultraviolet phosphorus from bone so as to maintain the normal blood
light on 7-dehydrocholesterol widely distributed in oily levels of calcium and phosphorus.
secretions of the skin. The vitamin so formed by irradiation iii) On kidneys. Vitamin D stimulates reabsorption of calcium
enters the body directly through the skin. Pigmentation of at distal renal tubular level, though this function is also
the skin reduces the beneficial effects of ultraviolet light. parathyroid hormone-dependent.
ii) Exogenous sources. The other source of vitamin D is diet 2. Antiproliferative effects. Vitamin D receptor is expressed
such as deep sea fish, fish oil, eggs, butter, milk, some plants on the parathyroid gland cells by which active form of
and grains. vitamin D causes antiproliferative action on parathyroid cells
Irrespective of the source of vitamin D, it must be conver- and suppresses the parathormone gene. Besides, vitamin D
ted to its active metabolites (25-hydroxy vitamin D and 1,25- receptor is also expressed on cells of organs which do not