
Page 307 - Textbook of Pathology, 6th Edition
P. 307
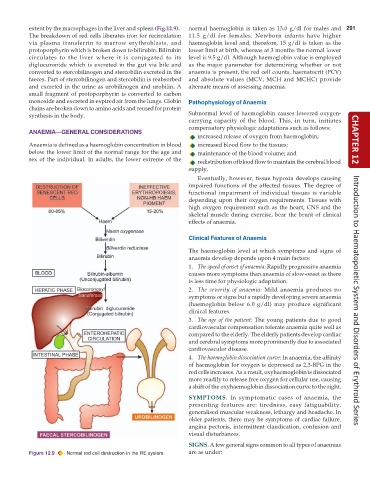
extent by the macrophages in the liver and spleen (Fig.12.9). normal haemoglobin is taken as 13.0 g/dl for males and 291
The breakdown of red cells liberates iron for recirculation 11.5 g/dl for females. Newborn infants have higher
via plasma transferrin to marrow erythroblasts, and haemoglobin level and, therefore, 15 g/dl is taken as the
protoporphyrin which is broken down to bilirubin. Bilirubin lower limit at birth, whereas at 3 months the normal lower
circulates to the liver where it is conjugated to its level is 9.5 g/dl. Although haemoglobin value is employed
diglucuronide which is excreted in the gut via bile and as the major parameter for determining whether or not
converted to stercobilinogen and stercobilin excreted in the anaemia is present, the red cell counts, haematocrit (PCV)
faeces. Part of stercobilinogen and stercobilin is reabsorbed and absolute values (MCV, MCH and MCHC) provide
and excreted in the urine as urobilinogen and urobilin. A alternate means of assessing anaemia.
small fragment of protoporphyrin is converted to carbon
monoxide and excreted in expired air from the lungs. Globin Pathophysiology of Anaemia
chains are broken down to amino acids and reused for protein
synthesis in the body. Subnormal level of haemoglobin causes lowered oxygen-
carrying capacity of the blood. This, in turn, initiates
compensatory physiologic adaptations such as follows:
ANAEMIA—GENERAL CONSIDERATIONS
increased release of oxygen from haemoglobin;
Anaemia is defined as a haemoglobin concentration in blood increased blood flow to the tissues; CHAPTER 12
below the lower limit of the normal range for the age and maintenance of the blood volume; and
sex of the individual. In adults, the lower extreme of the redistribution of blood flow to maintain the cerebral blood
supply.
Eventually, however, tissue hypoxia develops causing
impaired functions of the affected tissues. The degree of
functional impairment of individual tissues is variable
depending upon their oxygen requirements. Tissues with
high oxygen requirement such as the heart, CNS and the
skeletal muscle during exercise, bear the brunt of clinical
effects of anaemia.
Clinical Features of Anaemia
The haemoglobin level at which symptoms and signs of
anaemia develop depends upon 4 main factors:
1. The speed of onset of anaemia: Rapidly progressive anaemia
causes more symptoms than anaemia of slow-onset as there
is less time for physiologic adaptation.
2. The severity of anaemia: Mild anaemia produces no
symptoms or signs but a rapidly developing severe anaemia
(haemoglobin below 6.0 g/dl) may produce significant Introduction to Haematopoietic System and Disorders of Erythroid Series
clinical features.
3. The age of the patient: The young patients due to good
cardiovascular compensation tolerate anaemia quite well as
compared to the elderly. The elderly patients develop cardiac
and cerebral symptoms more prominently due to associated
cardiovascular disease.
4. The haemoglobin dissociation curve: In anaemia, the affinity
of haemoglobin for oxygen is depressed as 2,3-BPG in the
red cells increases. As a result, oxyhaemoglobin is dissociated
more readily to release free oxygen for cellular use, causing
a shift of the oxyhaemoglobin dissociation curve to the right.
SYMPTOMS. In symptomatic cases of anaemia, the
presenting features are: tiredness, easy fatiguability,
generalised muscular weakness, lethargy and headache. In
older patients, there may be symptoms of cardiac failure,
angina pectoris, intermittent claudication, confusion and
visual disturbances.
SIGNS. A few general signs common to all types of anaemias
Figure 12.9 Normal red cell destruction in the RE system. are as under: