
Page 647 - Textbook of Pathology, 6th Edition
P. 647
1. Intrahepatic portal hypertension. Cirrhosis is by far the 631
commonest cause of portal hypertension. Other less frequent
intrahepatic causes are metastatic tumours, non-cirrhotic
nodular regenerative conditions, hepatic venous obstruction
(Budd-Chiari syndrome), veno-occlusive disease,
schistosomiasis, diffuse granulomatous diseases and
extensive fatty change. In cirrhosis and other conditions,
there is obstruction to the portal venous flow by fibrosis,
thrombosis and pressure by regenerative nodules. About 30-
60% patients of cirrhosis develop significant portal
hypertension.
2. Posthepatic portal hypertension. This is uncommon and
results from obstruction to the blood flow through hepatic
vein into inferior vena cava. The causes are neoplastic
occlusion and thrombosis of the hepatic vein or of the inferior
vena cava (including Budd-Chiari syndrome). Prolonged
congestive heart failure and constrictive pericarditis may also
cause portal hypertension by transmitting the elevated
pressure through the hepatic vessels into the portal vein.
3. Prehepatic portal hypertension. Blockage of portal flow
before portal blood reaches the hepatic sinusoids results in
prehepatic portal hypertension. Such conditions are
thrombosis and neoplastic obstruction of the portal vein
before it ramifies in the liver, myelofibrosis, and congenital
absence of portal vein.
MAJOR SEQUELAE OF PORTAL HYPERTENSION. CHAPTER 21
Irrespective of the mechanisms involved in the pathogenesis
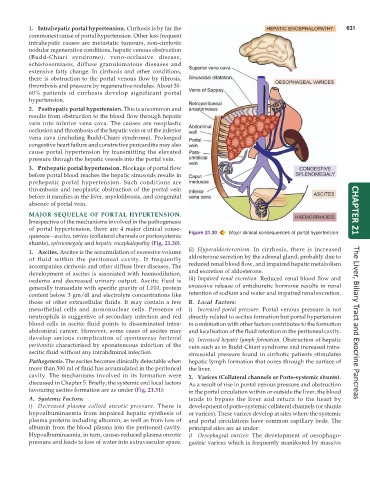
of portal hypertension, there are 4 major clinical conse-
quences—ascites, varices (collateral channels or portosystemic Figure 21.30 Major clinical consequences of portal hypertension.
shunts), splenomegaly and hepatic encephalopathy (Fig. 21.30).
ii) Hyperaldosteronism. In cirrhosis, there is increased
1. Ascites. Ascites is the accumulation of excessive volume
of fluid within the peritoneal cavity. It frequently aldosterone secretion by the adrenal gland, probably due to
accompanies cirrhosis and other diffuse liver diseases. The reduced renal blood flow, and impaired hepatic metabolism
development of ascites is associated with haemodilution, and excretion of aldosterone.
oedema and decreased urinary output. Ascitic fluid is iii) Impaired renal excretion. Reduced renal blood flow and
generally transudate with specific gravity of 1.010, protein excessive release of antidiuretic hormone results in renal
content below 3 gm/dl and electrolyte concentrations like retention of sodium and water and impaired renal excretion.
those of other extracellular fluids. It may contain a few B. Local Factors:
mesothelial cells and mononuclear cells. Presence of i) Increased portal pressure. Portal venous pressure is not
neutrophils is suggestive of secondary infection and red directly related to ascites formation but portal hypertension
blood cells in ascitic fluid points to disseminated intra- in combination with other factors contributes to the formation The Liver, Biliary Tract and Exocrine Pancreas
abdominal cancer. However, some cases of ascites may and localisation of the fluid retention in the peritoneal cavity.
develop serious complication of spontaneous bacterial ii) Increased hepatic lymph formation. Obstruction of hepatic
peritonitis characterised by sponateneous infection of the vein such as in Budd-Chiari syndrome and increased intra-
ascitic fluid without any intrabdminal infection. sinusoidal pressure found in cirrhotic patients stimulates
Pathogenesis. The ascites becomes clinically detectable when hepatic lymph formation that oozes through the surface of
more than 500 ml of fluid has accumulated in the peritoneal the liver.
cavity. The mechanisms involved in its formation were 2. Varices (Collateral channels or Porto-systemic shunts).
discussed in Chapter 5. Briefly, the systemic and local factors As a result of rise in portal venous pressure and obstruction
favouring ascites formation are as under (Fig. 21.31): in the portal circulation within or outside the liver, the blood
A. Systemic Factors: tends to bypass the liver and return to the heart by
i) Decreased plasma colloid oncotic pressure. There is development of porto-systemic collateral channels (or shunts
hypoalbuminaemia from impaired hepatic synthesis of or varices). These varices develop at sites where the systemic
plasma proteins including albumin, as well as from loss of and portal circulations have common capillary beds. The
albumin from the blood plasma into the peritoneal cavity. principal sites are as under:
Hypoalbuminaemia, in turn, causes reduced plasma oncotic i) Oesophageal varices: The development of oesophago-
pressure and leads to loss of water into extravascular space. gastric varices which is frequently manifested by massive