
Page 648 - Textbook of Pathology, 6th Edition
P. 648
632
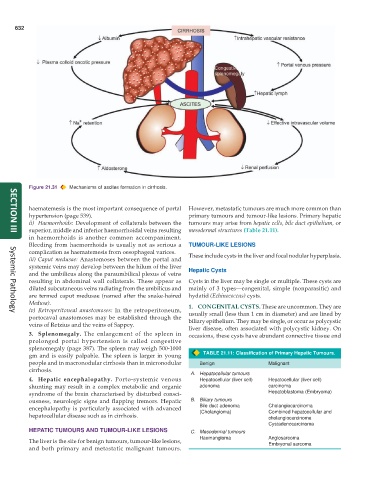
Figure 21.31 Mechanisms of ascites formation in cirrhosis.
haematemesis is the most important consequence of portal However, metastatic tumours are much more common than
hypertension (page 539). primary tumours and tumour-like lesions. Primary hepatic
ii) Haemorrhoids: Development of collaterals between the tumours may arise from hepatic cells, bile duct epithelium, or
superior, middle and inferior haemorrhoidal veins resulting mesodermal structures (Table 21.11).
SECTION III
in haemorrhoids is another common accompaniment.
Bleeding from haemorrhoids is usually not as serious a TUMOUR-LIKE LESIONS
complication as haematemesis from oesophageal varices. These include cysts in the liver and focal nodular hyperplasia.
iii) Caput medusae: Anastomoses between the portal and
systemic veins may develop between the hilum of the liver Hepatic Cysts
and the umbilicus along the paraumbilical plexus of veins
resulting in abdominal wall collaterals. These appear as Cysts in the liver may be single or multiple. These cysts are
dilated subcutaneous veins radiating from the umbilicus and mainly of 3 types—congenital, simple (nonparasitic) and
are termed caput medusae (named after the snake-haired hydatid (Echinococcus) cysts.
Medusa). 1. CONGENITAL CYSTS. These are uncommon. They are
iv) Retroperitoneal anastomoses: In the retroperitoneum, usually small (less than 1 cm in diameter) and are lined by
Systemic Pathology
portocaval anastomoses may be established through the biliary epithelium. They may be single, or occur as polycystic
veins of Retzius and the veins of Sappey.
liver disease, often associated with polycystic kidney. On
3. Splenomegaly. The enlargement of the spleen in occasions, these cysts have abundant connective tissue and
prolonged portal hypertension is called congestive
splenomegaly (page 387). The spleen may weigh 500-1000
gm and is easily palpable. The spleen is larger in young TABLE 21.11: Classification of Primary Hepatic Tumours.
people and in macronodular cirrhosis than in micronodular Benign Malignant
cirrhosis.
A. Hepatocellular tumours
4. Hepatic encephalopathy. Porto-systemic venous Hepatocellular (liver cell) Hepatocellular (liver cell)
shunting may result in a complex metabolic and organic adenoma carcinoma
syndrome of the brain characterised by disturbed consci- Hepatoblastoma (Embryoma)
ousness, neurologic signs and flapping tremors. Hepatic B. Biliary tumours
encephalopathy is particularly associated with advanced Bile duct adenoma Cholangiocarcinoma
hepatocellular disease such as in cirrhosis. (Cholangioma) Combined hepatocellular and
cholangiocarcinoma
Cystadenocarcinoma
HEPATIC TUMOURS AND TUMOUR-LIKE LESIONS C. Mesodermal tumours
Haemangioma Angiosarcoma
The liver is the site for benign tumours, tumour-like lesions, Embryonal sarcoma
and both primary and metastatic malignant tumours.