
Page 724 - Textbook of Pathology, 6th Edition
P. 724
708
SECTION III
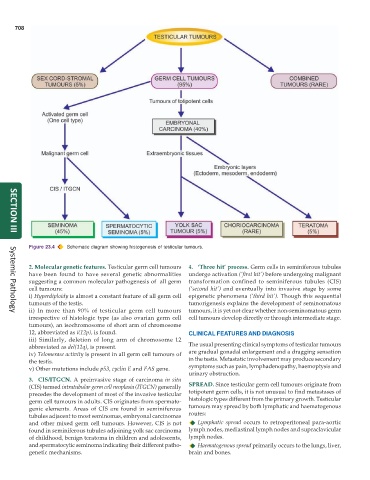
Figure 23.4 Schematic diagram showing histogenesis of testicular tumours.
2. Molecular genetic features. Testicular germ cell tumours 4. ‘Three hit’ process. Germ cells in seminiferous tubules
have been found to have several genetic abnormalities undergo activation (‘first hit’) before undergoing malignant
suggesting a common molecular pathogenesis of all germ transformation confined to seminiferous tubules (CIS)
cell tumours: (‘second hit’) and eventually into invasive stage by some
i) Hyperdiploidy is almost a constant feature of all germ cell epigenetic phenomena (‘third hit’). Though this sequential
tumours of the testis. tumorigenesis explains the development of seminomatous
ii) In more than 90% of testicular germ cell tumours tumours, it is yet not clear whether non-seminomatous germ
Systemic Pathology
irrespective of histologic type (as also ovarian germ cell cell tumours develop directly or through intermediate stage.
tumours), an isochromosome of short arm of chromosome
12, abbreviated as i(12p), is found. CLINICAL FEATURES AND DIAGNOSIS
iii) Similarly, deletion of long arm of chromosome 12
abbreviated as del(12q), is present. The usual presenting clinical symptoms of testicular tumours
iv) Telomerase activity is present in all germ cell tumours of are gradual gonadal enlargement and a dragging sensation
the testis. in the testis. Metastatic involvement may produce secondary
v) Other mutations include p53, cyclin E and FAS gene. symptoms such as pain, lymphadenopathy, haemoptysis and
urinary obstruction.
3. CIS/ITGCN. A preinvasive stage of carcinoma in situ
(CIS) termed intratubular germ cell neoplasia (ITGCN) generally SPREAD. Since testicular germ cell tumours originate from
precedes the development of most of the invasive testicular totipotent germ cells, it is not unusual to find metastases of
germ cell tumours in adults. CIS originates from spermato- histologic types different from the primary growth. Testicular
genic elements. Areas of CIS are found in seminiferous tumours may spread by both lymphatic and haematogenous
tubules adjacent to most seminomas, embryonal carcinomas routes:
and other mixed germ cell tumours. However, CIS is not Lymphatic spread occurs to retroperitoneal para-aortic
found in seminiferous tubules adjoining yolk sac carcinoma lymph nodes, mediastinal lymph nodes and supraclavicular
of childhood, benign teratoma in children and adolescents, lymph nodes.
and spermatocytic seminoma indicating their different patho- Haematogenous spread primarily occurs to the lungs, liver,
genetic mechanisms. brain and bones.