
Page 393 - First Aid for the USMLE Step 1 2020, Thirtieth edition [MedicalBooksVN.com]_Neat
P. 393
EndocrinE ` endocrine—PAthology EndocrinE ` endocrine—PAthology SEcTion iii 349
Adrenal insufficiency Inability of adrenal glands to generate enough glucocorticoids +/− mineralocorticoids for the body’s
needs. Symptoms include weakness, fatigue, orthostatic hypotension, muscle aches, weight loss, GI
disturbances, sugar and/or salt cravings. Treatment: glucocorticoid/mineralocorticoid replacement.
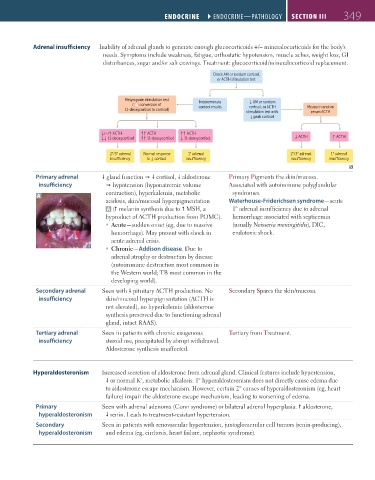
Check AM or random cortisol,
or ACTH stimulation test
Metyrapone stimulation test Indeterminate ↓ AM or random
( conversion of cortisol results cortisol, or ACTH Measure random
11-deoxycortisol to cortisol) stimulation test with serum ACTH
↓ peak cortisol
↓/−/↑ ACTH ↑↑ ACTH ↑↑ ACTH
↓↓ 11-deoxycortisol ↑↑ 11-deoxycortisol ↓ 11-deoxycortisol ↓ ACTH ↑ ACTH
2°/3° adrenal Normal response 1° adrenal 2°/3° adrenal 1° adrenal
insu ciency to ↓ cortisol insu ciency insu ciency insu ciency
Primary adrenal gland function cortisol, aldosterone Primary Pigments the skin/mucosa.
insufficiency hypotension (hyponatremic volume Associated with autoimmune polyglandular
A contraction), hyperkalemia, metabolic syndromes.
acidosis, skin/mucosal hyperpigmentation Waterhouse-Friderichsen syndrome—acute
A ( melanin synthesis due to MSH, a 1° adrenal insufficiency due to adrenal
byproduct of ACTH production from POMC). hemorrhage associated with septicemia
Acute—sudden onset (eg, due to massive (usually Neisseria meningitidis), DIC,
hemorrhage). May present with shock in endotoxic shock.
acute adrenal crisis.
Chronic—Addison disease. Due to
adrenal atrophy or destruction by disease
(autoimmune destruction most common in
the Western world; TB most common in the
developing world).
Secondary adrenal Seen with pituitary ACTH production. No Secondary Spares the skin/mucosa.
insufficiency skin/mucosal hyperpigmentation (ACTH is
not elevated), no hyperkalemia (aldosterone
synthesis preserved due to functioning adrenal
gland, intact RAAS).
Tertiary adrenal Seen in patients with chronic exogenous Tertiary from Treatment.
insufficiency steroid use, precipitated by abrupt withdrawal.
Aldosterone synthesis unaffected.
Hyperaldosteronism Increased secretion of aldosterone from adrenal gland. Clinical features include hypertension,
+
or normal K , metabolic alkalosis. 1° hyperaldosteronism does not directly cause edema due
to aldosterone escape mechanism. However, certain 2° causes of hyperaldosteronism (eg, heart
failure) impair the aldosterone escape mechanism, leading to worsening of edema.
Primary Seen with adrenal adenoma (Conn syndrome) or bilateral adrenal hyperplasia. aldosterone,
hyperaldosteronism renin. Leads to treatment-resistant hypertension.
Secondary Seen in patients with renovascular hypertension, juxtaglomerular cell tumors (renin-producing),
hyperaldosteronism and edema (eg, cirrhosis, heart failure, nephrotic syndrome).
FAS1_2019_08-Endocrine.indd 349 11/7/19 4:30 PM