
Page 714 - First Aid for the USMLE Step 1 2020, Thirtieth edition [MedicalBooksVN.com]_Neat
P. 714
670 seCtioN iii RespiRatoRy ` RESPIRATORY—PhYSIOlOgY RespiRatoRy ` RESPIRATORY—PAThOlOgY
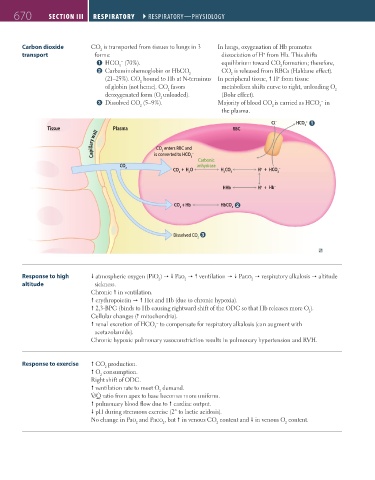
Carbon dioxide CO is transported from tissues to lungs in 3 In lungs, oxygenation of Hb promotes
2
transport forms: dissociation of H from Hb. This shifts
+
1 HCO (70%). equilibrium toward CO formation; therefore,
−
3
2
2 Carbaminohemoglobin or HbCO CO is released from RBCs (Haldane effect).
2
2
(21–25%). CO bound to Hb at N-terminus In peripheral tissue, H from tissue
+
2
of globin (not heme). CO favors metabolism shifts curve to right, unloading O
2
2
deoxygenated form (O unloaded). (Bohr effect).
2
3 Dissolved CO (5–9%). Majority of blood CO is carried as HCO in
−
2 2 3
the plasma.
Cl – HCO 3 – 1
Tissue Plasma RBC
Capillary wall CO enters RBC and
2
–
is converted to HCO
3
Carbonic
CO anhydrase
2
CO + H O H CO H + HCO –
+
2 2 2 3 3
HHb H + Hb –
+
CO + Hb HbCO 2
2
2
Dissolved CO 3
2
Response to high atmospheric oxygen (PiO ) Pao ventilation Paco respiratory alkalosis altitude
2
2
2
altitude sickness.
Chronic in ventilation.
erythropoietin Hct and Hb (due to chronic hypoxia).
2,3-BPG (binds to Hb causing rightward shift of the ODC so that Hb releases more O ).
2
Cellular changes ( mitochondria).
−
renal excretion of HCO to compensate for respiratory alkalosis (can augment with
3
acetazolamide).
Chronic hypoxic pulmonary vasoconstriction results in pulmonary hypertension and RVH.
Response to exercise CO production.
2
O consumption.
2
Right shift of ODC.
ventilation rate to meet O demand.
2
˙ ˙
V/Q ratio from apex to base becomes more uniform.
pulmonary blood flow due to cardiac output.
pH during strenuous exercise (2° to lactic acidosis).
No change in Pao and Paco , but in venous CO content and in venous O content.
2
2
2
2
FAS1_2019_16-Respiratory.indd 670 11/8/19 7:34 AM