
Page 469 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 469
CHAPTER 40: Pericardial Disease 339
or collapse of the right atrium and right ventricle, ventricular septal intrapericardial pressure will be elevated and should be equal to the
shifting with respiration, and enlargement of the inferior vena cava. intracardiac end-diastolic pressure.
7
With Doppler echocardiography, respiratory variation in mitral inflow
can be detected early in the evolution of tamponade. Moreover, the ■ PERICARDIOCENTESIS
8
changes in mitral inflow are highly sensitive, and may precede changes Pericardiocentesis historically was performed in a blinded or ECG-
in cardiac output, blood pressure, and other echocardiographic evi- guided fashion, usually from the subxyphoid approach. Although these
dence of tamponade. Respiratory changes in mitral inflow resolve after techniques may still be useful in some situations (eg, emergencies or car-
pericardiocentesis unless effusive-constrictive physiology is present. diogenic shock), the incidence of complications is high and echocardio-
■ INVASIVE HEMODYNAMICS graphic guidance is strongly preferred. Of note, care should be taken to
9
In patients with cardiac tamponade, the atrial pressure tracing typically avoid pericardiocentesis in the treatment of tamponade that occurs with
aortic dissection. In these patients, abrupt return of ventricular ejection
is elevated with prominent x descents and blunted or absent y descents may exacerbate the dissection and precipitate acute decompensation in
(Fig. 40-3). Preservation of the x descent occurs because systolic ejection these patients. 10
leads to a decrease in intracardiac volume and a temporary reduction
in right atrial and intrapericardial pressures. During the remainder of • Echocardiography is used to determine the most appropriate por-
the cardiac cycle, elevated intrapericardial pressure impairs ventricular tal of entry and needle direction into the pericardial effusion. The
filling leading to blunting or obliteration of the y descent. Corresponding window closest to the effusion usually is selected (Fig. 40-4). The
changes are also seen in ventricular pressure tracings with elevated most commonly used site is apical, but locations that have been used
diastolic pressures and loss or blunting of early diastolic pressure include axillary, left or right parasternal, and the subxyphoid window.
(or ventricular minimum pressure). The blunting or loss of the early With the imaging probe in place, the needle trajectory should be
rapid ventricular filling wave is the hallmark of cardiac tamponade that transfixed in the operator’s mind. Care should be taken to avoid the
distinguishes it from other diastolic filling disorders. Other hemody- internal mammary or intercostal arteries. The entry site is marked
namic findings include equalization of end-diastolic pressures, reduced with an indelible pen, followed by antiseptic cleansing, draping, and
cardiac output, and alterations in the systolic ejection period or pulse local anesthesia.
pressure that result from decreased stroke volume and are analogous • Using the predetermined site and angulation, a Polytef-sheathed nee-
to the bedside finding of pulsus paradoxus. During pericardiocentesis, dle is inserted at the entry site and advanced with gentle aspiration
80
FA
40
RA a
x v
120
FA
80
80
RA a v y
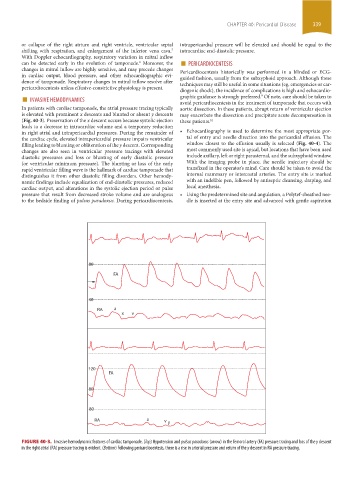
FIGURE 40-3. Invasive hemodynamic features of cardiac tamponade. (Top) Hypotension and pulsus paradoxus (arrow) in the femoral artery (FA) pressure tracing and loss of the y descent
in the right atrial (RA) pressure tracing is evident. (Bottom) Following pericardiocentesis, there is a rise in arterial pressure and return of the y descent in RA pressure tracing.
section03.indd 339 1/23/2015 2:07:42 PM