
Page 206 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 206
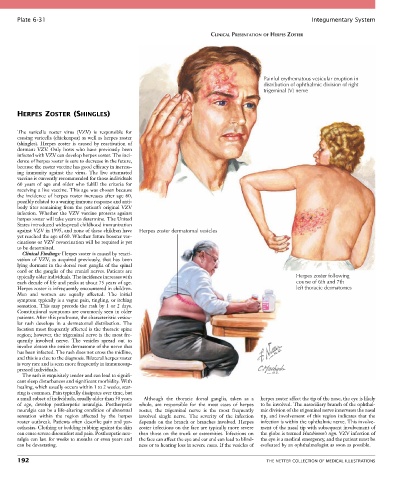
Plate 6-31 Integumentary System
CLINICAL PRESENTATION OF HERPES ZOSTER
Painful erythematous vesicular eruption in
distribution of ophthalmic division of right
trigeminal (V) nerve
HERPES ZOSTER (SHINGLES)
The varicella zoster virus (VZV) is responsible for
causing varicella (chickenpox) as well as herpes zoster
(shingles). Herpes zoster is caused by reactivation of
dormant VZV. Only hosts who have previously been
infected with VZV can develop herpes zoster. The inci-
dence of herpes zoster is sure to decrease in the future,
because the zoster vaccine has good efficacy in increas-
ing immunity against the virus. The live attenuated
vaccine is currently recommended for those individuals
60 years of age and older who fulfill the criteria for
receiving a live vaccine. This age was chosen because
the incidence of herpes zoster increases after age 60,
possibly related to a waning immune response and anti-
body titer remaining from the patient’s original VZV
infection. Whether the VZV vaccine protects against
herpes zoster will take years to determine. The United
States introduced widespread childhood immunization
against VZV in 1995, and none of these children have Herpes zoster dermatomal vesicles
yet reached the age of 60. Whether future booster vac-
cinations or VZV revaccination will be required is yet
to be determined.
Clinical Findings: Herpes zoster is caused by reacti-
vation of VZV, as acquired previously, that has been
lying dormant in the dorsal root ganglia of the spinal
cord or the ganglia of the cranial nerves. Patients are
typically older individuals. The incidence increases with Herpes zoster following
each decade of life and peaks at about 75 years of age. course of 6th and 7th
Herpes zoster is infrequently encountered in children. left thoracic dermatomes
Men and women are equally affected. The initial
symptom typically is a vague pain, tingling, or itching
sensation. This may precede the rash by 1 or 2 days.
Constitutional symptoms are commonly seen in older
patients. After this prodrome, the characteristic vesicu-
lar rash develops in a dermatomal distribution. The
location most frequently affected is the thoracic spine
region; however, the trigeminal nerve is the most fre-
quently involved nerve. The vesicles spread out to
involve almost the entire dermatome of the nerve that
has been infected. The rash does not cross the midline,
and this is a clue to the diagnosis. Bilateral herpes zoster
is very rare and is seen more frequently in immunosup-
pressed individuals.
The rash is exquisitely tender and can lead to signifi-
cant sleep disturbances and significant morbidity. With
healing, which usually occurs within 1 to 2 weeks, scar-
ring is common. Pain typically dissipates over time, but
a small subset of individuals, usually older than 50 years Although the thoracic dorsal ganglia, taken as a herpes zoster affect the tip of the nose, the eye is likely
of age, develop postherpetic neuralgia. Postherpetic whole, are responsible for the most cases of herpes to be involved. The nasociliary branch of the ophthal-
neuralgia can be a life-altering condition of abnormal zoster, the trigeminal nerve is the most frequently mic division of the trigeminal nerve innervates the nasal
sensation within the region affected by the herpes involved single nerve. The severity of the infection tip, and involvement of this region indicates that the
zoster outbreak. Patients often describe pain and par- depends on the branch or branches involved. Herpes infection is within the ophthalmic nerve. This involve-
esthesias. Clothing or bedding rubbing against the skin zoster infections on the face are typically more severe ment of the nasal tip with subsequent involvement of
can cause severe discomfort and pain. Postherpetic neu- than those on the trunk or extremities. Infections on the globe is termed Hutchinson’s sign. VZV infection of
ralgia can last for weeks to months or even years and the face can affect the eye and ear and can lead to blind- the eye is a medical emergency, and the patient must be
can be devastating. ness or to hearing loss in severe cases. If the vesicles of evaluated by an ophthalmologist as soon as possible.
192 THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS