
Page 203 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 203
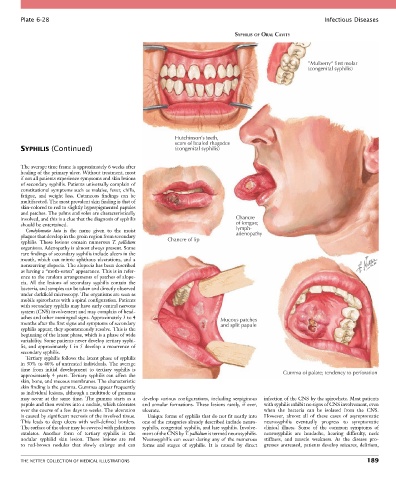
Plate 6-28 Infectious Diseases
SYPHILIS OF ORAL CAVITY
”Mulberry“ first molar
(congenital syphilis)
Hutchinson’s teeth,
scars of healed rhagades
SYPHILIS (Continued) (congenital syphilis)
The average time frame is approximately 6 weeks after
healing of the primary ulcer. Without treatment, most
if not all patients experience symptoms and skin lesions
of secondary syphilis. Patients universally complain of
constitutional symptoms such as malaise, fever, chills,
fatigue, and weight loss. Cutaneous findings can be
multifaceted. The most prevalent skin finding is that of
skin-colored to red to slightly hyperpigmented papules
and patches. The palms and soles are characteristically
involved, and this is a clue that the diagnosis of syphilis Chancre
should be entertained. of tongue;
Condylomata lata is the name given to the moist lymph-
plaques that develop in the groin region from secondary adenopathy
syphilis. These lesions contain numerous T. pallidum Chancre of lip
organisms. Adenopathy is almost always present. Some
rare findings of secondary syphilis include ulcers in the
mouth, which can mimic aphthous ulcerations, and a
nonscarring alopecia. The alopecia has been described
as having a “moth-eaten” appearance. This is in refer-
ence to the random arrangements of patches of alope-
cia. All the lesions of secondary syphilis contain the
bacteria, and samples can be taken and directly observed
under darkfield microscopy. The organisms are seen as
mobile spirochetes with a spiral configuration. Patients
with secondary syphilis may have early central nervous
system (CNS) involvement and may complain of head-
aches and other meningeal signs. Approximately 3 to 4 Mucous patches
months after the first signs and symptoms of secondary and split papule
syphilis appear, they spontaneously resolve. This is the
beginning of the latent phase, which is a phase of wide
variability. Some patients never develop tertiary syphi-
lis, and approximately 1 in 5 develop a recurrence of
secondary syphilis.
Tertiary syphilis follows the latent phase of syphilis
in 30% to 40% of untreated individuals. The average
time from initial development to tertiary syphilis is Gumma of palate; tendency to perforation
approximately 4 years. Tertiary syphilis can affect the
skin, bone, and mucous membranes. The characteristic
skin finding is the gumma. Gummas appear frequently
as individual lesions, although a multitude of gummas
may occur at the same time. The gumma starts as a develop various configurations, including serpiginous infection of the CNS by the spirochete. Most patients
papule and then evolves into a nodule, which ulcerates and annular formations. These lesions rarely, if ever, with syphilis exhibit no signs of CNS involvement, even
over the course of a few days to weeks. The ulceration ulcerate. when the bacteria can be isolated from the CNS.
is caused by significant necrosis of the involved tissue. Unique forms of syphilis that do not fit neatly into However, almost all of these cases of asymptomatic
This leads to deep ulcers with well-defined borders. one of the categories already described include neuro- neurosyphilis eventually progress to symptomatic
The surface of the ulcer may be covered with gelatinous syphilis, congenital syphilis, and late syphilis. Involve- clinical illness. Some of the common symptoms of
exudates. Another form of tertiary syphilis is the ment of the CNS by T. pallidum is termed neurosyphilis. neurosyphilis are headache, hearing difficulty, neck
nodular syphilid skin lesion. These lesions are red Neurosyphilis can occur during any of the numerous stiffness, and muscle weakness. As the disease pro-
to red-brown nodules that slowly enlarge and can forms and stages of syphilis. It is caused by direct gresses untreated, patients develop seizures, delirium,
THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS 189