
Page 215 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 215
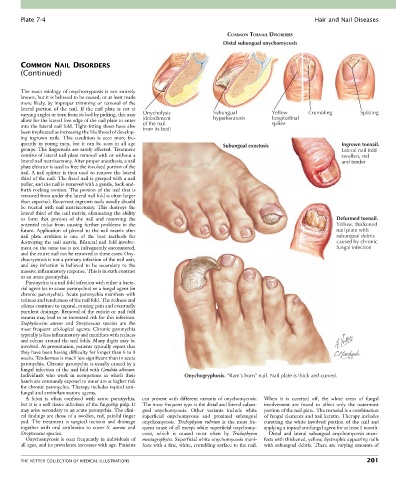
Plate 7-4 Hair and Nail Diseases
COMMON TOENAIL DISORDERS
Distal subungual onychomycosis
COMMON NAIL DISORDERS
(Continued)
The exact etiology of onychocryptosis is not entirely
known, but it is believed to be caused, or at least made
more likely, by improper trimming or removal of the
lateral portion of the nail. If the nail plate is cut at
varying angles or torn from its bed by picking, this may Onycholysis Subungual Yellow Crumbling Splitting
allow for the lateral free edge of the nail plate to enter (detachment hyperkeratosis longitudinal
spikes
into the lateral nail fold. Tight-fitting shoes have also of the nail
from its bed)
been implicated as increasing the likelihood of develop-
ing ingrown nails. This condition is seen more fre-
quently in young men, but it can be seen in all age Subungual exostosis Ingrown toenail.
groups. The fingernails are rarely affected. Treatment Lateral nail fold
consists of lateral nail plate removal with or without a swollen, red
lateral nail matrixectomy. After proper anesthesia, a nail and tender
plate elevator is used to free the involved portion of the
nail. A nail splitter is then used to remove the lateral
third of the nail. The freed nail is grasped with a nail
puller, and the nail is removed with a gentle, back-and-
forth rocking motion. The portion of the nail that is
removed from under the lateral nail fold is often larger
than expected. Recurrent ingrown nails usually should
be treated with nail matrixectomy. This destroys the
lateral third of the nail matrix, eliminating the ability
to form that portion of the nail and removing the Deformed toenail.
potential nidus from causing further problems in the Yellow, thickened
future. Application of phenol to the nail matrix after nail plate with
nail plate avulsion is one of the best methods for subungual debris
destroying the nail matrix. Bilateral nail fold involve- caused by chronic
ment on the same toe is not infrequently encountered, fungal infection
and the entire nail can be removed in these cases. Ony-
chocryptosis is not a primary infection of the nail unit,
and any infection is believed to be secondary to the
massive inflammatory response. This is in stark contrast
to an acute paronychia.
Paronychia is a nail fold infection with either a bacte-
rial agent (as in acute paronychia) or a fungal agent (in
chronic paronychia). Acute paronychia manifests with
redness and tenderness of the nail fold. The redness and
edema continue to expand, causing pain and eventually
purulent drainage. Removal of the cuticle or nail fold
trauma may lead to an increased risk for this infection.
Staphylococcus aureus and Streptococcus species are the
most frequent etiological agents. Chronic paronychia
typically is less inflammatory and manifests with redness
and edema around the nail folds. Many digits may be
involved. At presentation, patients typically report that
they have been having difficulty for longer than 6 to 8
weeks. Tenderness is much less significant than in acute
paronychia. Chronic paronychia is usually caused by a
fungal infection of the nail fold with Candida albicans.
Individuals who work in occupations in which their Onychogryphosis. “Ram’s horn” nail. Nail plate is thick and curved.
hands are constantly exposed to water are at higher risk
for chronic paronychia. Therapy includes topical anti-
fungal and antiinflammatory agents.
A felon is often confused with acute paronychia, can present with different variants of onychomycosis. When it is curetted off, the white areas of fungal
but it is a soft tissue infection of the fingertip pulp. It The most frequent type is the distal and lateral subun- involvement are found to affect only the outermost
may arise secondary to an acute paronychia. The clini- gual onychomycosis. Other variants include white portion of the nail plate. The material is a combination
cal findings are those of a swollen, red, painful finger superficial onychomycosis and proximal subungual of fungal elements and nail keratin. Therapy includes
pad. The treatment is surgical incision and drainage onychomycosis. Trichophyton rubrum is the most fre- curetting the white involved portion of the nail and
together with oral antibiotics to cover S. aureus and quent cause of all except white superficial onychomy- applying a topical antifungal agent for at least 1 month.
Streptococcus species. cosis, which is caused most often by Trichophyton Distal and lateral subungual onychomycosis mani-
Onychomycosis is seen frequently in individuals of mentagrophytes. Superficial white onychomycosis mani- fests with thickened, yellow, dystrophic appearing nails
all ages, and its prevalence increases with age. Patients fests with a fine, white, crumbling surface to the nail. with subungual debris. There are varying amounts of
THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS 201