
Page 219 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 219
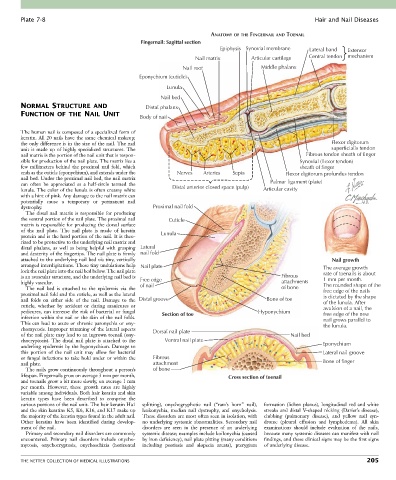
Plate 7-8 Hair and Nail Diseases
ANATOMY OF THE FINGERNAIL AND TOENAIL
Fingernail: Sagittal section
Epiphysis Synovial membrane Lateral band Extensor
Nail matrix Articular cartilage Central tendon mechanism
Nail root Middle phalanx
Eponychium (cuticle)
Lunula
Nail bed
NORMAL STRUCTURE AND Distal phalanx
FUNCTION OF THE NAIL UNIT
Body of nail
The human nail is composed of a specialized form of
keratin. All 20 nails have the same chemical makeup;
the only difference is in the size of the nail. The nail Flexor digitorum
unit is made up of highly specialized structures. The superficialis tendon
nail matrix is the portion of the nail unit that is respon- Fibrous tendon sheath of finger
sible for production of the nail plate. The matrix lies a Synovial (flexor tendon)
few millimeters behind the proximal nail fold, which sheath of finger
ends as the cuticle (eponychium), and extends under the Nerves Arteries Septa Flexor digitorum profundus tendon
nail bed. Under the proximal nail bed, the nail matrix
can often be appreciated as a half-circle termed the Distal anterior closed space (pulp) Palmar ligament (plate)
lunula. The color of the lunula is often creamy white Articular cavity
with a hint of pink. Any damage to the nail matrix can
potentially cause a temporary or permanent nail
dystrophy. Proximal nail fold
The distal nail matrix is responsible for producing
the ventral portion of the nail plate. The proximal nail Cuticle
matrix is responsible for producing the dorsal surface
of the nail plate. The nail plate is made of keratin Lunula
protein and is the hard portion of the nail. It is theo-
rized to be protective to the underlying nail matrix and
distal phalanx, as well as being helpful with grasping Lateral
and dexterity of the fingertips. The nail plate is firmly nail fold
attached to the underlying nail bed via tiny, vertically Nail growth
arranged interdigitations. These tiny undulations help Nail plate The average growth
lock the nail plate into the nail bed below. The nail plate rate of toenails is about
is an avascular structure, and the underlying nail bed is Free edge Fibrous 1 mm per month.
highly vascular. of nail attachments The rounded shape of the
The nail bed is attached to the epidermis via the of bone free edge of the nails
proximal nail fold and the cuticle, as well as the lateral is dictated by the shape
nail folds on either side of the nail. Damage to the Distal groove Bone of toe of the lunula. After
cuticle, whether by accident or during manicures or avulsion of a nail, the
pedicures, can increase the risk of bacterial or fungal Section of toe Hyponychium free edge of the new
infection within the nail or the skin of the nail folds. nail grows parallel to
This can lead to acute or chronic paronychia or ony- the lunula.
chomycosis. Improper trimming of the lateral aspects Dorsal nail plate
of the nail plate may lead to an ingrown toenail (ony- Nail bed
chocryptosis). The distal nail plate is attached to the Ventral nail plate
underling epidermis by the hyponychium. Damage to Eponychium
this portion of the nail unit may allow for bacterial Lateral nail groove
or fungal infections to take hold under or within the Fibrous
nail plate. attachment Bone of finger
The nails grow continuously throughout a person’s of bone
lifespan. Fingernails grow on average 3 mm per month, Cross section of toenail
and toenails grow a bit more slowly, on average 1 mm
per month. However, these growth rates are highly
variable among individuals. Both hair keratin and skin
keratin types have been described to comprise the
various portions of the nail unit. The hair keratin Ha1 splitting), onychogryphotic nail (“ram’s horn” nail), formation (lichen planus), longitudinal red and white
and the skin keratins K5, K6, K16, and K17 make up leukonychia, median nail dystrophy, and onycholysis. streaks and distal V-shaped nicking (Darier’s disease),
the majority of the keratin types found in the adult nail. These disorders are most often seen in isolation, with clubbing (pulmonary disease), and yellow nail syn-
Other keratins have been identified during develop- no underlying systemic abnormalities. Secondary nail drome (pleural effusion and lymphedema). All skin
ment of the nail. disorders are seen in the presence of an underlying examinations should include evaluation of the nails,
Primary and secondary nail disorders are commonly systemic disease; examples include koilonychia (caused because many systemic diseases can manifest with nail
encountered. Primary nail disorders include onycho- by iron deficiency), nail plate pitting (many conditions findings, and these clinical signs may be the first signs
mycosis, onychocryptosis, onychoschizia (horizontal including psoriasis and alopecia areata), pterygium of underlying disease.
THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS 205