
Page 224 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 224
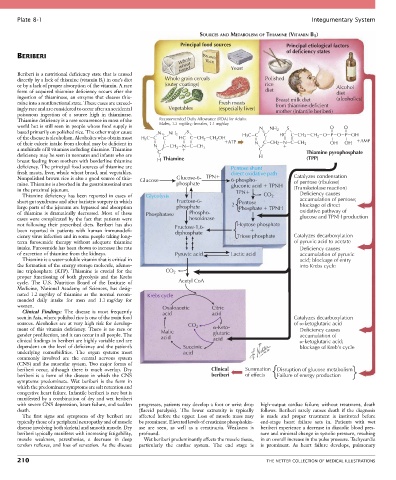
Plate 8-1 Integumentary System
SOURCES AND METABOLISM OF THIAMINE (VITAMIN B )
1
Principal food sources Principal etiological factors
of deficiency states
BERIBERI Brown
Whole Rice
wheat
Beriberi is a nutritional deficiency state that is caused bread Yeast
directly by a lack of thiamine (vitamin B 1 ) in one’s diet Whole grain cereals Polished
or by a lack of proper absorption of the vitamin. A rare (outer coatings) rice Alcohol
form of acquired thiamine deficiency occurs after the diet diet
ingestion of thiaminase, an enzyme that cleaves thia- Breast milk diet (alcoholics)
mine into a nonfunctional state. These cases are exceed- Fresh meats from thiamine-deficient
ingly rare and are considered to occur after an accidental Vegetables (especially liver) mother (infantile beriberi)
poisonous ingestion of a source high in thiaminase.
Thiamine deficiency is a rare occurrence in most of the Recommended Daily Allowance (RDA) for Adults:
world but is still seen in people whose food supply is Males, 1.2 mg/day; females, 1.1 mg/day N NH
based primarily on polished rice. The other major cause NH 2 S 2 HC S O O
2
of the disease is alcoholism. Alcoholics who obtain most H C C N C HC C CH CH OH H3C C C C CH2 CH O P O P OH
2
2
3
of their caloric intake from alcohol may be deficient in C CH N C CH ATP N C CH2 N C CH 3 OH OH AMP
a multitude of B vitamins including thiamine. Thiamine N C 2 3 C Thiamine pyrophosphate
deficiency may be seen in neonates and infants who are H (TPP)
breast feeding from mothers with borderline thiamine H Thiamine
deficiency. The principal food sources of thiamine are Pentose shunt
fresh meats, liver, whole wheat bread, and vegetables. direct oxidative path
Nonpolished brown rice is also a good source of thia- Glucose Glucose-6- TPN 6-phospho- Catalyzes condensation
mine. Thiamine is absorbed in the gastrointestinal tract phosphate gluconic acid TPNH of pentose (ribulose)
in the proximal jejunum. TPN (Transketolase reaction)
Thiamine deficiency has been reported in cases of Glycolysis CO 2 Deficiency causes
short gut syndrome and after bariatric surgery in which Fructose-6- Pentose accumulation of pentose;
large parts of the jejunum are bypassed and absorption phosphate 2 Phosphate TPNH blockage of direct
of thiamine is dramatically decreased. Most of these Phosphatase Phospho- oxidative pathway of
cases were complicated by the fact that patients were hexokinase glucose and TPNH production
not following their prescribed diets. Beriberi has also Fructose-1,6- Heptose phosphate
been reported in patients with human immunodefi- diphosphate
ciency virus infection and in some people taking long- Triose phosphate Catalyzes decarboxylation
term furosemide therapy without adequate thiamine of pyruvic acid to acetate
intake. Furosemide has been shown to increase the rate Deficiency causes
of excretion of thiamine from the kidneys. Pyruvic acid Lactic acid accumulation of pyruvic
Thiamine is a water-soluble vitamin that is critical in acid; blockage of entry
the formation of the energy storage molecule, adenos- into Krebs cycle
ine triphosphate (ATP). Thiamine is crucial for the CO 2
proper functioning of both glycolysis and the Krebs
cycle. The U.S. Nutrition Board of the Institute of Acetyl CoA
Medicine, National Academy of Sciences, has desig-
nated 1.2 mg/day of thiamine as the normal recom- Krebs cycle
mended daily intake for men and 1.1 mg/day for
women. Oxaloacetic Citric
Clinical Findings: The disease is most frequently acid acid
seen in Asia, where polished rice is one of the main food Catalyzes decarboxylation
sources. Alcoholics are at very high risk for develop- CO 2 of -ketoglutaric acid
ment of this vitamin deficiency. There is no race or Malic -Keto- Deficiency causes
gender predilection, and it can occur in all people. The acid glutaric accumulation of
clinical findings in beriberi are highly variable and are acid -ketoglutaric acid;
dependent on the level of deficiency and the patient’s Succinic blockage of Kreb’s cycle
underlying comorbidities. The organ systems most acid
commonly involved are the central nervous system
(CNS) and the muscular system. Two major forms of
beriberi occur, although there is much overlap. Dry Clinical Summation Disruption of glucose metabolism
beriberi is a form of the disease in which the CNS beriberi of effects Failure of energy production
symptoms predominate. Wet beriberi is the form in
which the predominant symptoms are salt retention and
congestive heart failure. Infantile beriberi is rare but is
manifested by a combination of dry and wet beriberi
with severe CNS depression, heart failure, and sudden progresses, patients may develop a foot or wrist drop high-output cardiac failure; without treatment, death
death. (flaccid paralysis). The lower extremity is typically follows. Beriberi rarely causes death if the diagnosis
The first signs and symptoms of dry beriberi are affected before the upper. Loss of muscle mass may is made and proper treatment is instituted before
typically those of a peripheral neuropathy and of muscle be prominent. Elevated levels of creatinine phosphokin- end-stage heart failure sets in. Patients with wet
disease involving both skeletal and smooth muscle. Dry ase are seen, as well as a creatinuria. Weakness is beriberi experience a decrease in diastolic blood pres-
beriberi typically manifests with increasing fatigability, profound. sure and minimal change in systolic pressure, resulting
muscle weakness, paresthesias, a decrease in deep Wet beriberi predominantly affects the muscle tissue, in an overall increase in the pulse pressure. Tachycardia
tendon reflexes, and loss of sensation. As the disease particularly the cardiac system. The end stage is is prominent. As heart failure develops, pulmonary
210 THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS