
Page 234 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 234
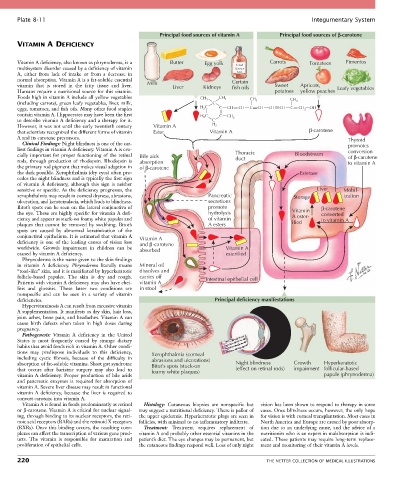
Plate 8-11 Integumentary System
Principal food sources of vitamin A Principal food sources of b-carotene
VITAMIN A DEFICIENCY
Vitamin A deficiency, also known as phrynoderma, is a Butter Egg yolk Cod Carrots Tomatoes Pimentos
multisystem disorder caused by a deficiency of vitamin Liver
A, either from lack of intake or from a decrease in Oil
normal absorption. Vitamin A is a fat-soluble essential Certain
vitamin that is stored in the fatty tissue and liver. Milk Liver Kidneys fish oils Sweet Apricots, Leafy vegetables
Humans require a nutritional source for this vitamin. potatoes yellow peaches
Foods high in vitamin A include all yellow vegetables CH 3 CH 3 CH CH
(including carrots), green leafy vegetables, liver, milk, C 3 3
eggs, tomatoes, and fish oils. Many other food staples H 2 C C CH CH C CH CH CH C CH 2 OH
contain vitamin A. Hippocrates may have been the first H 2 C C CH
to describe vitamin A deficiency and a therapy for it. C 3
However, it was not until the early twentieth century Vitamin A H 2
that scientists recognized the different forms of vitamin Ester Vitamin A β−carotene
A and its carotene precursors. Thyroid
Clinical Findings: Night blindness is one of the ear- promotes
liest findings in vitamin A deficiency. Vitamin A is cru- conversion
cially important for proper functioning of the retinal Bile aids Thoracic Bloodstream of β−carotene
rods, through production of rhodopsin. Rhodopsin is absorption duct to vitamin A
the primary rod pigment that makes visual adaption in of β−carotene
the dark possible. Xerophthalmia (dry eyes) often pre- Esterase
cedes the night blindness and is typically the first sign
of vitamin A deficiency, although this sign is neither
sensitive or specific. As the deficiency progresses, the Liver Mobil-
xerophthalmia may result in corneal dryness, abrasions, Pancreatic Storage ization
ulceration, and keratomalacia, which leads to blindness. secretions
Bitot’s spots can be seen on the lateral conjunctiva of promote β−carotene
the eye. These are highly specific for vitamin A defi- hydrolysis Vitamin converted
ciency and appear as stuck-on foamy white papules and of vitamin A ester- to vitamin A
plaques that cannot be removed by swabbing. Bitot’s A esters ified
spots are caused by abnormal keratinization of the
conjunctival epithelium. It is estimated that vitamin A Vitamin A
deficiency is one of the leading causes of vision loss and β −carotene
worldwide. Growth impairment in children can be absorbed Vitamin A
caused by vitamin A deficiency. esterified
Phrynoderma is the name given to the skin findings
in vitamin A deficiency. Phrynoderma literally means Mineral oil
“toad-like” skin, and it is manifested by hyperkeratotic dissolves and
follicle-based papules. The skin is dry and rough. carries off Intestinal epithelial cell
Patients with vitamin A deficiency may also have chei- vitamin A
litis and glossitis. These latter two conditions are in stool
nonspecific and can be seen in a variety of vitamin
deficiencies. Principal deficiency manifestations
Hypervitaminosis A can result from excessive vitamin
A supplementation. It manifests as dry skin, hair loss,
joint aches, bone pain, and headaches. Vitamin A can
cause birth defects when taken in high doses during
pregnancy.
Pathogenesis: Vitamin A deficiency in the United
States is most frequently caused by strange dietary
habits that avoid foods rich in vitamin A. Other condi-
tions may predispose individuals to this deficiency, Xerophthalmia (corneal
including cystic fibrosis, because of the difficulty in abrasions and ulcerations)
absorption of fat-soluble vitamins. Short gut syndrome Bitot’s spots (stuck-on Night blindness Growth Hyperkeratotic
that occurs after bariatric surgery may also lead to foamy white plaques) (effect on retinal rods) impairment follicular-based
vitamin A deficiency. Proper production of bile acids papule (phrynoderma)
and pancreatic enzymes is required for absorption of
vitamin A. Severe liver disease may result in functional
vitamin A deficiency, because the liver is required to
convert carotene into vitamin A.
Vitamin A is found in foods predominantly as retinol Histology: Cutaneous biopsies are nonspecific but vision has been shown to respond to therapy in some
or β-carotene. Vitamin A is critical for nuclear signal- may suggest a nutritional deficiency. There is pallor of cases. Once blindness occurs, however, the only hope
ing, through binding to its nuclear receptors, the reti- the upper epidermis. Hyperkeratotic plugs are seen in for vision is with corneal transplantation. Most cases in
noic acid receptors (RARs) and the retinoid X receptors follicles, with minimal to no inflammatory infiltrate. North America and Europe are caused by poor absorp-
(RXRs). Once this binding occurs, the resulting com- Treatment: Treatment requires replacement of tion due to an underlying cause, and the advice of a
plexes can affect the transcription of various gene prod- vitamin A and probably other essential vitamins in the nutritionist who is an expert in malabsorption is indi-
ucts. The vitamin is responsible for maturation and patient’s diet. The eye changes may be permanent, but cated. These patients may require long-term replace-
proliferation of epithelial cells. the cutaneous findings respond well. Loss of only night ment and monitoring of their vitamin A levels.
220 THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS