
Page 48 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 48
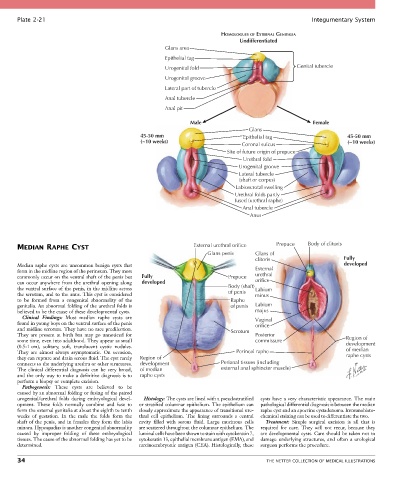
Plate 2-21 Integumentary System
HOMOLOGUES OF EXTERNAL GENITALIA
Undifferentiated
Glans area
Epithelial tag
Urogenital fold Genital tubercle
Urogenital groove
Lateral part of tubercle
Anal tubercle
Anal pit
Male Female
Glans
45-50 mm Epithelial tag 45-50 mm
(~10 weeks) (~10 weeks)
Coronal sulcus
Site of future origin of prepuce
Urethral fold
Urogenital groove
Lateral tubercle
(shaft or corpus)
Labioscrotal swelling
Urethral folds partly
fused (urethral raphe)
Anal tubercle
Anus
MEDIAN RAPHE CYST External urethral orifice Prepuce Body of clitoris
Glans penis Glans of
clitoris Fully
Median raphe cysts are uncommon benign cysts that developed
form in the midline region of the perineum. They most External
commonly occur on the ventral shaft of the penis but Fully Prepuce urethral
can occur anywhere from the urethral opening along developed orifice
the ventral surface of the penis, in the midline across Body (shaft) Labium
the scrotum, and to the anus. This cyst is considered of penis minus
to be formed from a congenital abnormality of the Raphe
genitalia. An abnormal folding of the urethral folds is of penis Labium
believed to be the cause of these developmental cysts. majus
Clinical Findings: Most median raphe cysts are Vaginal
found in young boys on the ventral surface of the penis orifice
and midline scrotum. They have no race predilection. Scrotum
They are present at birth but may go unnoticed for Posterior
some time, even into adulthood. They appear as small commissure Region of
(0.5-1 cm), solitary, soft, translucent cystic nodules. development
They are almost always asymptomatic. On occasion, Perineal raphe of median
they can rupture and drain serous fluid. The cyst rarely Region of raphe cysts
connects to the underlying urethra or other structures. development Perianal tissues (including
The clinical differential diagnosis can be very broad, of median external anal sphincter muscle)
and the only way to make a definitive diagnosis is to raphe cysts
perform a biopsy or complete excision.
Pathogenesis: These cysts are believed to be
caused by an abnormal folding or fusing of the paired
urogenital/urethral folds during embryological devel- Histology: The cysts are lined with a pseudostratified cysts have a very characteristic appearance. The main
opment. These folds normally combine and fuse to or stratified columnar epithelium. The epithelium can pathological differential diagnosis is between the median
form the external genitalia at about the eighth to tenth closely approximate the appearance of transitional ure- raphe cyst and an apocrine cystadenoma. Immunohisto-
weeks of gestation. In the male the folds form the thral cell epithelium. The lining surrounds a central chemical staining can be used to differentiate the two.
shaft of the penis, and in females they form the labia cavity filled with serous fluid. Large mucinous cells Treatment: Simple surgical excision is all that is
minora. Hypospadias is another congenital abnormality are scattered throughout the columnar epithelium. The required for cure. They will not recur, because they
caused by improper folding of these embryological luminal cells have been shown to stain with cytokeratin 7, are developmental cysts. Care should be taken not to
tissues. The cause of the abnormal folding has yet to be cytokeratin 13, epithelial membrane antigen (EMA), and damage underlying structures, and often a urological
determined. carcinoembryonic antigen (CEA). Histologically, these surgeon performs the procedure.
34 THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS