
Page 336 - Cardiac Nursing
P. 336
xd
xd
q
q
6
g
e 3
6
12
12
0-3
A
e 3
q
32.
32.
0:3
0:3
1
1
M
M
0 P
0 P
Pa
Pa
g
g
/09
/09
/29
/29
c.
c.
15_
In
a
a
In
15_
LWB
LWB
LWBK340-c15_ pp300-332.qxd 6/29/09 10:30 PM Page 312 Aptara Inc.
K34
0-c
0-c
K34
p
A
p
p
p
30
0-3
p
30
t
ara
ara
t
312 P A R T III / Assessment of Heart Disease
2
V 6
2 2 2 2 2 2 2 2 2 2 2
I
1 1 1 1 1 1 1 1
V
A 2 1 B
VR
VRR
aVV
VR
aV
a a a a a a a a
R R R R R R R R
V
V V V V V
R
VR
V
I I I I I aV R V V V V V V V V V V 1 1 1 1 V V V V V V V V V V V V V V V 4 4 4 4 4 4 4 4
VLL
VL
VL
V V V V
V
a a a a a a a a a a
aVV
L L L L L L
I I I I I I I I I II aV L V V V V V V V V 2 2 2 2 2 2 2 2 2 2 2 V V V V V V V V V V V V 5 5 5 5 5 5 5 5
a aV
VF
V
F
VF
VF
V
VFF
V V V V V
aV
I I I I I I I I I I I I I I I I III aV F F F F F F F F V V V V V V V V V V 3 3 3 3 3 3 3 3 3 3 3 V V V V V V V V V V V V V V V 6 6 6 6 6 6 6 6
aVV
a a a a a a a a
C
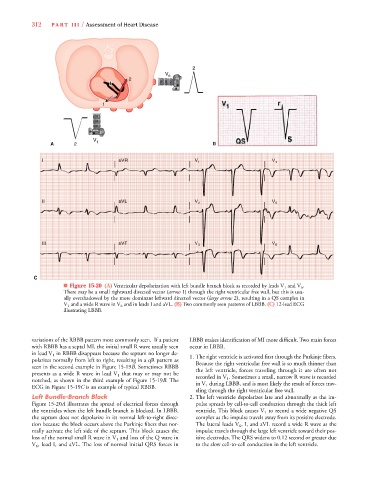
■ Figure 15-20 (A) Ventricular depolarization with left bundle branch block as recorded by leads V 1 and V 6 .
There may be a small rightward directed vector (arrow 1) through the right ventricular free wall, but this is usu-
ally overshadowed by the more dominant leftward directed vector (large arrow 2), resulting in a QS complex in
V 1 and a wide R wave in V 6 and in leads I and aVL. (B) Two commonly seen patterns of LBBB. (C) 12-lead ECG
illustrating LBBB.
variations of the RBBB pattern most commonly seen. If a patient LBBB makes identification of MI more difficult. Two main forces
with RBBB has a septal MI, the initial small R wave usually seen occur in LBBB.
in lead V 1 in RBBB disappears because the septum no longer de-
1. The right ventricle is activated first through the Purkinje fibers.
polarizes normally from left to right, resulting in a qR pattern as
Because the right ventricular free wall is so much thinner than
seen in the second example in Figure 15-19B. Sometimes RBBB
the left ventricle, forces traveling through it are often not
presents as a wide R wave in lead V 1 that may or may not be
recorded in V 1 . Sometimes a small, narrow R wave is recorded
notched, as shown in the third example of Figure 15-19B. The
in V 1 during LBBB, and is most likely the result of forces trav-
ECG in Figure 15-19C is an example of typical RBBB.
eling through the right ventricular free wall.
Left Bundle-Branch Block 2.The left ventricle depolarizes late and abnormally as the im-
0
Figure 15-20A illustrates the spread of electrical forces through pulse spreads by cell-to-cell conduction through the thick left
0
the ventricles when the left bundle branch is blocked. In LBBB, ventricle. This block causes V 1 to record a wide negative QS
the septum does not depolarize in its normal left-to-right direc- complex as the impulse travels away from its positive electrode.
tion because the block occurs above the Purkinje fibers that nor- The lateral leads V 6 , I, and aVL record a wide R wave as the
mally activate the left side of the septum. This block causes the impulse travels through the large left ventricle toward their pos-
loss of the normal small R wave in V 1 and loss of the Q wave in itive electrodes. The QRS widens to 0.12 second or greater due
V 6 , lead I, and aVL. The loss of normal initial QRS forces in to the slow cell-to-cell conduction in the left ventricle.