
Page 353 - Cardiac Nursing
P. 353
1
0:3
1
/09
/09
0:3
M
Pa
M
0 P
0 P
q
q
q
32.
32.
xd
/29
/29
6
xd
6
Pa
t
p
t
ara
ara
p
29
29
A
p
A
e 3
e 3
g
g
g
c.
a
a
In
c.
In
30
K34
K34
LWB
LWB
30
0-c
15_
15_
p
p
0-c
0-3
0-3
LWBK340-c15_ pp300-332.qxd 6/29/09 10:30 PM Page 329 Aptara Inc.
C HAPTER 1 5 / Electrocardiography 329
V1
V1
V1
V V1
V4
V4
V4
aVR
V V
R
aVR
I I I I I aVR V 1 V4 4 4
V
aVR
V
a aVR
aVL
aVL
a aVL
III I II II a aVL V2 2 2 2 2 2 2 2 V5 5 5 5
L
V
V
V2
V V V5
V5
V V V2
V3
aVF
V3 3
V3
V
V V V3
V
V V V3
V
V V V6
V6
aVF FVFVFVVF
aVF
V V V6
V6
III II I III II I III II I III III III a aVF V V V3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 V6 6 6 6 6 6 6
V V V6
a aVF
aVF
aVF
a aVF
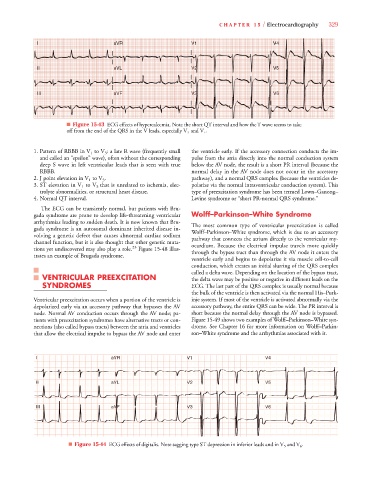
■ Figure 15-43 ECG effects of hypercalcemia. Note the short QT interval and how the T wave seems to take
off from the end of the QRS in the V leads, especially V 3 and V 4 .
V
1. Pattern of RBBB in V 1 to V 3 : a late R wave (frequently small the ventricle early. If the accessory connection conducts the im-
and called an “epsilon” wave), often without the corresponding pulse from the atria directly into the normal conduction system
deep S wave in left ventricular leads that is seen with true below the AV node, the result is a short PR interval (because the
RBBB. normal delay in the AV node does not occur in the accessory
2. J point elevation in V 1 to V 3 . pathway), and a normal QRS complex (because the ventricles de-
3. ST elevation in V 1 to V 3 that is unrelated to ischemia, elec- polarize via the normal intraventricular conduction system). This
trolyte abnormalities, or structural heart disease. type of preexcitation syndrome has been termed Lown–Ganong–
4. Normal QT interval. Levine syndrome or “short PR-normal QRS syndrome.”
The ECG can be transiently normal, but patients with Bru-
gada syndrome are prone to develop life-threatening ventricular Wolff–Parkinson–White Syndrome
arrhythmias leading to sudden death. It is now known that Bru- The most common type of ventricular preexcitation is called
gada syndrome is an autosomal dominant inherited disease in- Wolff–Parkinson–White syndrome, which is due to an accessory
volving a genetic defect that causes abnormal cardiac sodium pathway that connects the atrium directly to the ventricular my-
channel function, but it is also thought that other genetic muta- ocardium. Because the electrical impulse travels more quickly
tions yet undiscovered may also play a role. 23 Figure 15-48 illus- through the bypass tract than through the AV node it enters the
trates an example of Brugada syndrome.
ventricle early and begins to depolarize it via muscle cell-to-cell
conduction, which creates an initial slurring of the QRS complex
called a delta wave. Depending on the location of the bypass tract,
VENTRICULAR PREEXCITATION the delta wave may be positive or negative in different leads on the
SYNDROMES ECG. The last part of the QRS complex is usually normal because
the bulk of the ventricle is then activated via the normal His–Purk-
Ventricular preexcitation occurs when a portion of the ventricle is inje system. If most of the ventricle is activated abnormally via the
depolarized early via an accessory pathway that bypasses the AV accessory pathway, the entire QRS can be wide. The PR interval is
node. Normal AV conduction occurs through the AV node; pa- short because the normal delay through the AV node is bypassed.
tients with preexcitation syndromes have alternative tracts or con- Figure 15-49 shows two examples of Wolff–Parkinson–White syn-
nections (also called bypass tracts) between the atria and ventricles drome. See Chapter 16 for more information on Wolff–Parkin-
that allow the electrical impulse to bypass the AV node and enter son–White syndrome and the arrhythmias associated with it.
V1
V1
V1
4 4 4 4 4 4 4 4 4 4 4 4
V V V V V V V V V V V V V V
V
VRR
VR
VR
V
V
VR
V V V V V V V V
aV
aV
R
I I I I a a a a a a a a aV R R R R R R R R V1 1 1 1 1 1 1 V V V V V V V V V V V V V V4
VL
V
V
VL
VL
VLL
V V V V V V V V
II II II II aV L L L L L L L L L V2 2 2 2 2 2 2 2 2 2 2 V V V V V V V V V V V V V V5
aV
aV
V
5 5 5 5 5 5 5 5 5 5 5 5
a a a a a a a a
V2
V V V V V V V V V V V V V V
V2
V2
aV
a a a a a a a a
V V V V V V V V
V
6 6 6 6 6 6 6 6 6
V
aV
I I I I II II II II aV F F F F F F F F F F F F F F V3 3 3 3 3 3 3 3 3 V V V V V V V V V V V V V V6
V
V
V
V
V
V
V
V
V
V V3
V V V V V V V V V V V V V V
V3
V
V
V
V
V
V
V
V
■ Figure 15-44 ECG effects of digitalis. Note sagging type ST depression in inferior leads and in V 5 and V 6 .