
Page 351 - Cardiac Nursing
P. 351
6
/29
xd
6
/29
/09
/09
p
A
p
32.
t
p
32.
q
xd
q
q
g
g
Pa
g
e 3
27
A
e 3
27
0:3
0:3
1
1
0 P
M
Pa
0 P
M
c.
LWB
c.
In
In
15_
LWB K34 0-c 15_ p p pp300-332.qxd 6/29/09 10:30 PM Page 327 Aptara Inc.
0-c
LWBK340-c15_
K34
ara
0-3
t
ara
0-3
a
a
30
30
C HAPTER 1 5 / Electrocardiography 327
V
V
V
aV
aV
a a a a a a a a
R R R R R R R R
V1
V11
I I I I I aV R V V V V V V V V V V V V V V V 1 1 1 1 V4
V1
R
VR
VR
VR
V1
V V V V V
VRR
V44
V4
V V V V V V V V V V V
4
4 4 4 4 4 4 4 4
V4
2 2 2 2 2
V V V V V V V V V V V V V V V
V2
V2
V2
V
VL
VLL
V
VL
VL
V V V V V
V
aV
a a a a a a a a
aV
I I I I II II II II II aV L L L L L L L L L V22 V5
5 5 5 5 5 5 5 5
5
V55
V5
V V V V V V V V V V V
V5
T T T T T T T T T T T T T T U U U U U U U U U U U U U U
I I I I II II II II II II II II III aV F F F F F F F F V3 V6
3 3 3 3 3
V3
F
V V V V V
aV
aV
a a a a a a a a
V3
V V V V V V V V V V V V V V V
V33
VF
V
V
VF
V
VFF
VF
6
6 6 6 6 6 6 6 6
V V V V V V V V V V V
V6
V66
V6
T T T T T T T T T T U U U U U U U U U U U U U U U
A I I I I V V V V V V V V V V
V1
V11
V V V V V V V V V V V
R R R R R R R R R R R R
R
V V V V V V V V V V V V V V V
V4
4
4
4 4 4 4
V V V V V V V V VR
V4
I I I I a a a a a a a a aV R V1 1 1 1 1 V4
V1
V4
U U U U U U U U U U U U U U U U U U U U U U U U U U
T T T T T T T T T T
5 5 5
5
V V V V V V V V V V V V
V5
5
V5
V V V V V V V V V
V2
V22
V V V V V V VL
I I I I I I I a a a a a a a a aV L L L L L L L V2 2 2 2 2 2 2 2 V5
V6
I I I II II II I I I I I a a a a a a a a aV F V V V V V V V V V 3 3 3 3 3 3 3 V6
6
V V V V V V V V V V V V
F
F F F F F F
V6
V33
V3
V3
V V V V V V VF
6 6 6
6
B
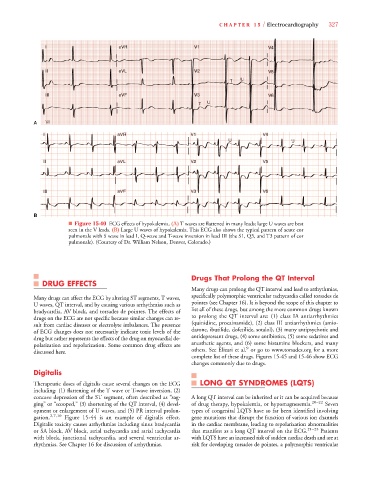
■ Figure 15-40 ECG effects of hypokalemia. (A) T waves are flattened in many leads; large U waves are best
seen in the V leads. (B) Large U waves of hypokalemia. This ECG also shows the typical pattern of acute cor
pulmonale with S wave in lead I, Q-wave and T-wave inversion in lead III (the S1, Q3, and T3 pattern of cor
pulmonale). (Courtesy of Dr. William Nelson, Denver, Colorado.)
Drugs That Prolong the QT Interval
DRUG EFFECTS
Many drugs can prolong the QT interval and lead to arrhythmias,
Many drugs can affect the ECG by altering ST segments, T waves, specifically polymorphic ventricular tachycardia called torsades de
U waves, QT interval, and by causing various arrhythmias such as pointes (see Chapter 16). It is beyond the scope of this chapter to
bradycardia, AV block, and torsades de pointes. The effects of list all of these drugs, but among the more common drugs known
drugs on the ECG are not specific because similar changes can re- to prolong the QT interval are: (1) class IA antiarrhythmics
sult from cardiac diseases or electrolyte imbalances. The presence (quinidine, procainamide), (2) class III antiarrhythmics (amio-
of ECG changes does not necessarily indicate toxic levels of the darone, ibutilide, dofetilide, sotalol), (3) many antipsychotic and
drug but rather represents the effects of the drug on myocardial de- antidepressant drugs, (4) some antibiotics, (5) some sedatives and
polarization and repolarization. Some common drug effects are anesthetic agents, and (6) some histamine blockers, and many
9
discussed here. others. See Elizari et al. or go to www.torsades.org for a more
complete list of these drugs. Figures 15-45 and 15-46 show ECG
changes commonly due to drugs.
Digitalis
Therapeutic doses of digitalis cause several changes on the ECG LONG QT SYNDROMES (LQTS)
including: (1) flattening of the T wave or T-wave inversion, (2)
concave depression of the ST segment, often described as “sag- A long QT interval can be inherited or it can be acquired because
ging” or “scooped,” (3) shortening of the QT interval, (4) devel- of drug therapy, hypokalemia, or hypomagnesemia. 20–22 Seven
opment or enlargement of U waves, and (5) PR interval prolon- types of congenital LQTS have so far been identified involving
gation. 2,7,10 Figure 15-44 is an example of digitalis effect. gene mutations that disrupt the function of various ion channels
Digitalis toxicity causes arrhythmias including sinus bradycardia in the cardiac membrane, leading to repolarization abnormalities
or SA block, AV block, atrial tachycardia and atrial tachycardia that manifest as a long QT interval on the ECG. 21–23 Patients
with block, junctional tachycardia, and several ventricular ar- with LQTS have an increased risk of sudden cardiac death and are at
rhythmias. See Chapter 16 for discussion of arrhythmias. risk for developing torsades de pointes, a polymorphic ventricular