
Page 395 - Cardiac Nursing
P. 395
2:1
6 A
2:1
1
1
6 A
Pa
Pa
Pa
M
M
1
xd
6
xd
q
q
6
/09
/09
/09
/30
/30
ara
ara
t
p
t
a
c.
c.
In
a
In
p
e 3
e 3
g
g
g
71
A
p
A
71
71
q
K34
33
LWB
K34
33
16_
16_
0-c
0-c
87.
87.
3-3
3-3
LWB
LWBK340-c16_ p p pp333-387.qxd 6/30/09 12:16 AM Page 371 Aptara Inc.
C HAPTER 1 6 / Arrhythmias and Conduction Disturbances 371
■ Figure 16-14 Monomorphic VT. Tracings show two different examples, each with QRS complexes of one
morphology.
Management of monomorphic VT is discussed earlier in this states that -blockers or calcium channel blockers may be effec-
chapter under the section titled “Ventricular Tachycardia”. tive drug therapy, and that catheter ablation is useful in patients
The term idiopathic VT refers to VT that occurs in people with who are drug refractory/intolerant or in those who do not desire
no structural heart disease. The most common type of idiopathic long-term drug therapy. 49 Table 16-5 summarizes the guidelines
VT arises in the RVOT, and is seen in 60% to 80% of patients for the management of VTs.
with VT and no structural heart disease. 22,48,52 RVOT tachycardia
presents with LBBB morphology and inferior axis, and occurs in Polymorphic VT
two forms: (1) nonsustained, repetitive monomorphic VT charac- PVT refers to VT with unstable, continuously varying QRS mor-
terized by frequent repetitive salvos of VT or (2) paroxysmal, phology often occurring at rates of approximately 200 beats per
sustained monomorphic VT induced by exercise. Both types can minute. It can occur in short repetitive salvos, longer sustained
be terminated by adenosine, supporting the hypothesis that the runs, or can degenerate into VF and cause SCD. PVT can be clas-
mechanism is triggered activity due to DADs. 52 Although most sified on the basis of whether it is associated with normal or pro-
adenosine-sensitive VTs originate from the RVOT, about 10% to longed QT intervals. Catecholaminergic PVT and short QT syn-
15% come from the left ventricular outflow tract. The ACC/AHA/ drome (SQTS) are two types of PVT in which the QT interval is
ESC practice guidelines for managing ventricular arrhythmias 49 normal or short. TdP is PVT that occurs in the presence of a long
recommend using -blockers, calcium channel blockers, and/or QT interval.
class IC antiarrhythmics if drug therapy is to be used for managing PVT with a normal QT interval can occur in the presence of
RVOT tachycardia; and catheter ablation in those who are drug in- ventricular ischemia during acute coronary syndrome or following
tolerant or do not desire long-term drug therapy. MI, although it is not a common arrhythmia. 76 Figure 16-15
Idiopathic left VT (also called fascicular tachycardia or verapamil- shows PVT in a patient during acute anterior wall MI. Therapy
sensitive VT) originates near the left posterior fascicle in the left for PVT associated with ischemia should be directed toward re-
ventricle and presents with RBBB morphology, superior axis, and lieving the ischemia by via either surgery or angioplasty. The
relatively narrow QRS complex ( 0.14 second). 22,48,52 The ACC/AHA/ESC practice guidelines for managing ventricular ar-
49
mechanism is thought to be reentry around the distal Purkinje rhythmias recommend IV -blockers for PVT if ischemia is sus-
network of the posterior fascicle. This is the one type of VT for pected. For recurrent PVT in the absence of a long QT interval,
which IV verapamil is effective therapy; normally verapamil is not IV amiodarone is useful and lidocaine may be helpful. Electrical
recommended in VT due to its ability to depress contractility and cardioversion is necessary for sustained PVT with hemodynamic
lead to further hemodynamic deterioration. The ACC/AHA/ compromise, and if the rhythm degenerates to VF, defibrillation is
ESC practice guidelines for managing ventricular arrhythmias required.
V 1
III
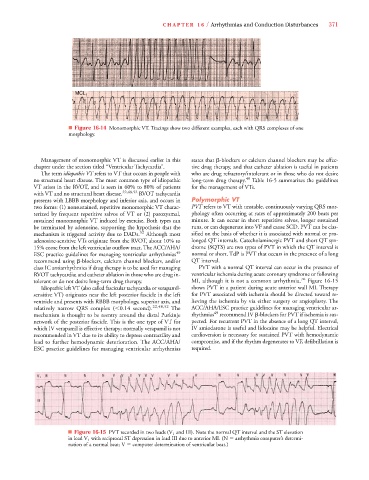
■ Figure 16-15 PVT recorded in two leads (V 1 and III). Note the normal QT interval and the ST elevation
in lead V 1 with reciprocal ST depression in lead III due to anterior MI. (N arrhythmia computer’s determi-
nation of a normal beat; V computer determination of ventricular beat.)