
Page 397 - Cardiac Nursing
P. 397
6 A
6 A
2:1
1
2:1
M
Pa
g
Pa
M
Pa
6
/30
6
xd
xd
/30
1
1
/09
/09
/09
ara
ara
t
p
t
a
c.
c.
In
a
In
e 3
73
e 3
g
g
73
p
p
A
73
A
q
33
33
p
3-3
3-3
LWB
p
0-c
K34
K34
16_
16_
0-c
87.
LWBK340-c16_ pp333-387.qxd 6/30/09 12:16 AM Page 373 Aptara Inc.
LWB
87.
q
q
C HAPTER 1 6 / Arrhythmias and Conduction Disturbances 373
MCL 1
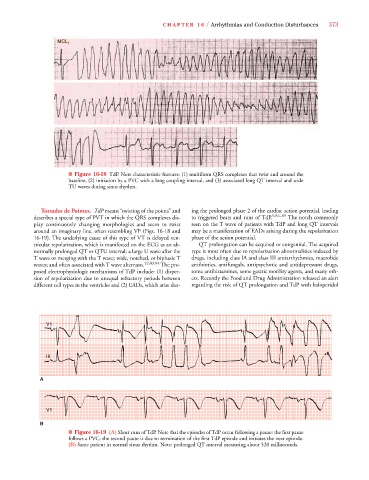
■ Figure 16-18 TdP. Note characteristic features: (1) multiform QRS complexes that twist and around the
baseline, (2) initiation by a PVC with a long coupling interval, and (3) associated long QT interval and wide
TU waves during sinus rhythm.
Torsades de Pointes. TdP means “twisting of the points” and ing the prolonged phase 2 of the cardiac action potential, leading
describes a special type of PVT in which the QRS complexes dis- to triggered beats and runs of TdP. 5,83–85 The notch commonly
play continuously changing morphologies and seem to twist seen on the T wave of patients with TdP and long QT intervals
around an imaginary line, often resembling VF (Figs. 16-18 and may be a manifestation of EADs arising during the repolarization
16-19). The underlying cause of this type of VT is delayed ven- phase of the action potential.
tricular repolarization, which is manifested on the ECG as an ab- QT prolongation can be acquired or congenital. The acquired
normally prolonged QT or QTU interval; a large U wave after the type is most often due to repolarization abnormalities induced by
T wave or merging with the T wave; wide, notched, or biphasic T drugs, including class IA and class III antiarrhythmics, macrolide
waves; and often associated with T wave alternans. 22,83,84 The pro- antibiotics, antifungals, antipsychotic and antidepressant drugs,
posed electrophysiologic mechanisms of TdP include: (1) disper- some antihistamines, some gastric motility agents, and many oth-
sion of repolarization due to unequal refractory periods between ers. Recently the Food and Drug Administration released an alert
different cell types in the ventricles and (2) EADs, which arise dur- regarding the risk of QT prolongation and TdP with haloperidol
V V1
V1
V1
III III
A
V1
V V V1
V V V V V V V1
V1
V1
V1
V V V1
B
■ Figure 16-19 (A) Short runs of TdP. Note that the episodes of TdP occur following a pause: the first pause
follows a PVC; the second pause is due to termination of the first TdP episode and initiates the next episode.
(B) Same patient in normal sinus rhythm. Note: prolonged QT interval measuring about 520 milliseconds.