
Page 400 - Cardiac Nursing
P. 400
1
1
2:1
/09
/09
1
M
M
Pa
2:1
6 A
6 A
q
q
xd
87.
87.
q
/30
/30
/09
xd
6
6
Pa
t
ara
ara
p
p
t
In
c.
c.
a
a
In
g
e 3
e 3
Pa
g
g
A
A
p
76
76
76
LWBK340-c16_
LWB K34 0-c 16_ p p pp333-387.qxd 6/30/09 12:16 AM Page 376 Aptara Inc.
33
LWB
16_
0-c
K34
33
3-3
3-3
376 P A R T III / Assessment of Heart Disease
V1
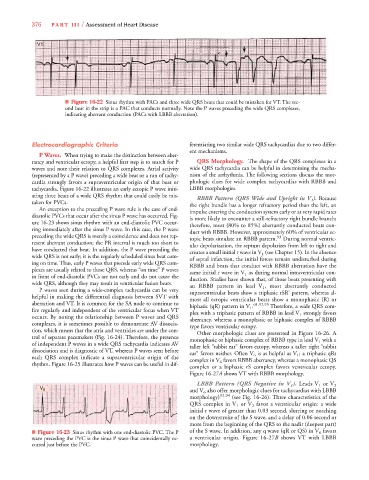
■ Figure 16-22 Sinus rhythm with PACs and three wide QRS beats that could be mistaken for VT. The sec-
ond beat in the strip is a PAC that conducts normally. Note the P waves preceding the wide QRS complexes,
indicating aberrant conduction (PACs with LBBB aberration).
Electrocardiographic Criteria ferentiating two similar wide QRS tachycardias due to two differ-
ent mechanisms.
P Waves. When trying to make the distinction between aber-
rancy and ventricular ectopy, a helpful first step is to search for P QRS Morphology. The shape of the QRS complexes in a
waves and note their relation to QRS complexes. Atrial activity wide QRS tachycardia can be helpful in determining the mecha-
(represented by a P wave) preceding a wide beat or a run of tachy- nism of the arrhythmia. The following sections discuss the mor-
cardia strongly favors a supraventricular origin of that beat or phologic clues for wide complex tachycardias with RBBB and
tachycardia. Figure 16-22 illustrates an early ectopic P wave initi- LBBB morphologies.
ating three beats of a wide QRS rhythm that could easily be mis- RBBB Pattern (QRS Wide and Upright in VV ). Because
V
1 1 1
taken for PVCs. the right bundle has a longer refractory period than the left, an
An exception to the preceding P wave rule is the case of end- impulse entering the conduction system early or at very rapid rates
diastolic PVCs that occur after the sinus P wave has occurred. Fig- is more likely to encounter a still-refractory right bundle branch;
ure 16-23 shows sinus rhythm with an end-diastolic PVC occur- therefore, most (80% to 85%) aberrantly conducted beats con-
ring immediately after the sinus P wave. In this case, the P wave duct with RBBB. However, approximately 60% of ventricular ec-
preceding the wide QRS is merely a coincidence and does not rep- topic beats simulate an RBBB pattern. 93 During normal ventric-
resent aberrant conduction; the PR interval is much too short to ular depolarization, the septum depolarizes from left to right and
have conducted that beat. In addition, the P wave preceding the creates a small initial r wave in V 1 (see Chapter 15). In the absence
wide QRS is not early; it is the regularly scheduled sinus beat com- of septal infarction, the initial forces remain undisturbed during
ing on time. Thus, early P waves that precede early wide QRS com- RBBB and beats that conduct with RBBB aberration have the
plexes are usually related to those QRS, whereas “on time” P waves same initial r wave in V 1 as during normal intraventricular con-
in front of end-diastolic PVCs are not early and do not cause the duction. Studies have shown that, of those beats presenting with
wide QRS, although they may result in ventricular fusion beats. an RBBB pattern in lead V 1 , most aberrantly conducted
P waves seen during a wide-complex tachycardia can be very supraventricular beats show a triphasic rSR’ pattern, whereas al-
helpful in making the differential diagnosis between SVT with most all ectopic ventricular beats show a monophasic (R) or
aberration and VT. It is common for the SA node to continue to biphasic (qR) pattern in V 1 . 61,92,93 Therefore, a wide QRS com-
fire regularly and independent of the ventricular focus when VT plex with a triphasic pattern of RBBB in lead V 1 strongly favors
occurs. By noting the relationship between P waves and QRS aberrancy, whereas a monophasic or biphasic complex of RBBB
complexes, it is sometimes possible to demonstrate AV dissocia- type favors ventricular ectopy.
tion, which means that the atria and ventricles are under the con- Other morphologic clues are presented in Figure 16-26. A
trol of separate pacemakers (Fig. 16-24). Therefore, the presence monophasic or biphasic complex of RBBB type in lead V 1 with a
of independent P waves in a wide QRS tachycardia indicates AV taller left “rabbit ear” favors ectopy, whereas a taller right “rabbit
dissociation and is diagnostic of VT, whereas P waves seen before ear” favors neither. Often V 6 is as helpful as V 1 ; a triphasic qRs
each QRS complex indicate a supraventricular origin of the complex in V 6 favors RBBB aberrancy, whereas a monophasic QS
rhythm. Figure 16-25 illustrates how P waves can be useful in dif-
complex or a biphasic rS complex favors ventricular ectopy.
7
7
Figure 16-27A shows VT with RBBB morphology.
1 1 1
LBBB Pattern (QRS Negative in VV ). Leads V 1 or V 2
V V 6 and V 6 also offer morphologic clues for tachycardias with LBBB
morphology) 92,94 (see Fig. 16-26). Three characteristics of the
QRS complex in V 1 or V 2 favor a ventricular origin: a wide
initial r wave of greater than 0.03 second, slurring or notching
on the downstroke of the S wave, and a delay of 0.06 second or
more from the beginning of the QRS to the nadir (deepest part)
■ Figure 16-23 Sinus rhythm with one end-diastolic PVC. The P of the S wave. In addition, any q wave (qR or QS) in V 6 favors
wave preceding the PVC is the sinus P wave that coincidentally oc- a ventricular origin. Figure 16-27B shows VT with LBBB
curred just before the PVC. morphology.