
Page 399 - Cardiac Nursing
P. 399
2:1
2:1
1
1
1
6 A
Pa
Pa
M
6 A
M
/09
xd
xd
q
q
q
6
/09
/09
/30
6
/30
Pa
ara
ara
t
p
t
a
c.
c.
In
a
In
p
e 3
e 3
g
g
g
75
A
p
A
75
75
16_
33
33
LWB K34 0-c 16_ p p pp333-387.qxd 6/30/09 12:16 AM Page 375 Aptara Inc.
LWB
LWBK340-c16_
0-c
87.
87.
3-3
K34
3-3
C HAPTER 1 6 / Arrhythmias and Conduction Disturbances 375
Beat 1 Beat 2 Beat 3
LBB
Short Cycle RBB
V V V1
V1
V1 1
LBB
R R R R
Long Cycle
RBB
r r r
s s s s
V1
V V V1
V1
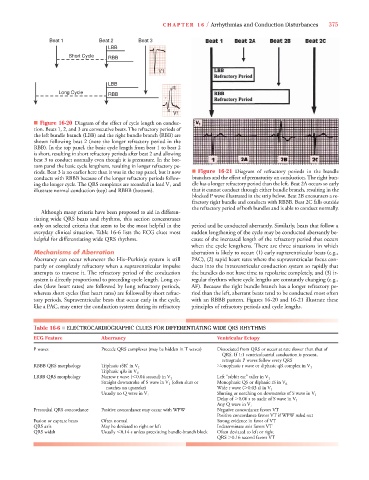
■ Figure 16-20 Diagram of the effect of cycle length on conduc-
tion. Beats 1, 2, and 3 are consecutive beats. The refractory periods of
the left bundle branch (LBB) and the right bundle branch (RBB) are
shown following beat 2 (note the longer refractory period in the
RBB). In the top panel, the basic cycle length from beat 1 to beat 2
is short, resulting in short refractory periods after beat 2 and allowing
beat 3 to conduct normally even though it is premature. In the bot-
tom panel the basic cycle lengthens, resulting in longer refractory pe-
riods. Beat 3 is no earlier here than it was in the top panel, but it now ■ Figure 16-21 Diagram of refractory periods in the bundle
conducts with RBBB because of the longer refractory periods follow- branches and the effect of prematurity on conduction. The right bun-
ing the longer cycle. The QRS complexes are recorded in lead V 1 and dle has a longer refractory period than the left. Beat 2A occurs so early
illustrate normal conduction (top) and RBBB (bottom). that it cannot conduct through either bundle branch, resulting in the
blocked P wave illustrated in the strip below. Beat 2B encounters a re-
fractory right bundle and conducts with RBBB. Beat 2C falls outside
the refractory period of both bundles and is able to conduct normally.
Although many criteria have been proposed to aid in differen-
tiating wide QRS beats and rhythms, this section concentrates
only on selected criteria that seem to be the most helpful in the period and be conducted aberrantly. Similarly, beats that follow a
everyday clinical situation. Table 16-6 lists the ECG clues most sudden lengthening of the cycle may be conducted aberrantly be-
helpful for differentiating wide QRS rhythms. cause of the increased length of the refractory period that occurs
when the cycle lengthens. There are three situations in which
Mechanisms of Aberration aberration is likely to occur: (1) early supraventricular beats (e.g.,
Aberrancy can occur whenever the His–Purkinje system is still PAC), (2) rapid heart rates where the supraventricular focus con-
partly or completely refractory when a supraventricular impulse ducts into the intraventricular conduction system so rapidly that
attempts to traverse it. The refractory period of the conduction the bundles do not have time to repolarize completely, and (3) ir-
system is directly proportional to preceding cycle length. Long cy- regular rhythms where cycle lengths are constantly changing (e.g.,
cles (slow heart rates) are followed by long refractory periods, AF). Because the right bundle branch has a longer refractory pe-
whereas short cycles (fast heart rates) are followed by short refrac- riod than the left, aberrant beats tend to be conducted most often
tory periods. Supraventricular beats that occur early in the cycle, with an RBBB pattern. Figures 16-20 and 16-21 illustrate these
like a PAC, may enter the conduction system during its refractory principles of refractory periods and cycle lengths.
Table 16-6 ■ ELECTROCARDIOGRAPHIC CLUES FOR DIFFERENTIATING WIDE QRS RHYTHMS
ECG Feature Aberrancy Ventricular Ectopy
P waves Precede QRS complexes (may be hidden in T waves) Dissociated from QRS or occur at rate slower than that of
QRS. If 1:1 ventriculoatrial conduction is present,
retrograde P waves follow every QRS
RBBB QRS morphology Triphasic rSR’ in V 1 Monophasic r wave or diphasic qR complex in V 1
Triphasic qRs in V 6
LBBB QRS morphology Narrow r wave ( 0.04 second) in V 1 Left “rabbit ear” taller in V 1
Straight downstroke of S wave in V 1 (often slurs or Monophasic QS or diphasic rS in V 6
notches on upstroke) Wide r wave ( 0.03 s) in V 1
Usually no Q wave in V 6 Slurring or notching on downstroke of S wave in V 1
Delay of 0.06 s to nadir of S wave in V 1
Any Q wave in V 6
Precordial QRS concordance Positive concordance may occur with WPW Negative concordance favors VT
Positive concordance favors VT if WPW ruled out
Fusion or capture beats Often normal Strong evidence in favor of VT
QRS axis May be deviated to right or left Indeterminate axis favors VT
QRS width Usually 0.14 s unless preexisting bundle-branch block Often deviated to left or right
QRS 0.16 second favors VT