
Page 401 - Cardiac Nursing
P. 401
1
1
2:1
/09
/09
1
M
M
Pa
2:1
6 A
6 A
q
q
xd
87.
87.
q
/30
/30
/09
xd
6
6
Pa
t
ara
ara
p
p
t
In
c.
c.
a
a
In
g
e 3
e 3
Pa
g
g
A
A
p
77
77
77
p
p
K34
33
33
16_
16_
0-c
K34
0-c
LWB
3-3
LWB
LWBK340-c16_ pp333-387.qxd 6/30/09 12:16 AM Page 377 Aptara Inc.
3-3
C HAPTER 1 6 / Arrhythmias and Conduction Disturbances 377
V 1
A
V 1
B
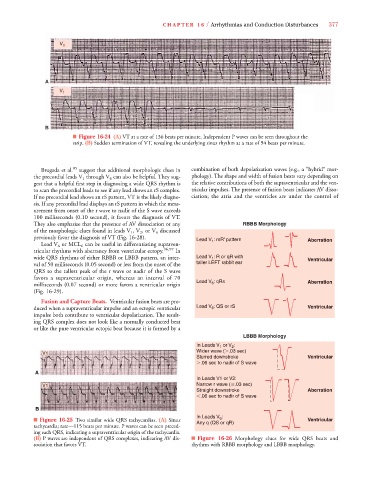
■ Figure 16-24 (A) VT at a rate of 136 beats per minute. Independent P waves can be seen throughout the
strip. (B) Sudden termination of VT, revealing the underlying sinus rhythm at a rate of 94 beats per minute.
Brugada et al. 95 suggest that additional morphologic clues in combination of both depolarization waves (e.g., a “hybrid” mor-
the precordial leads V 1 through V 6 can also be helpful. They sug- phology). The shape and width of fusion beats vary depending on
gest that a helpful first step in diagnosing a wide QRS rhythm is the relative contributions of both the supraventricular and the ven-
to scan the precordial leads to see if any lead shows an rS complex. tricular impulses. The presence of fusion beats indicates AV disso-
If no precordial lead shows an rS pattern, VT is the likely diagno- ciation; the atria and the ventricles are under the control of
sis. If any precordial lead displays an rS pattern in which the meas-
urement from onset of the r wave to nadir of the S wave exceeds
100 milliseconds (0.10 second), it favors the diagnosis of VT.
They also emphasize that the presence of AV dissociation or any RBBB Morphology
of the morphologic clues found in leads V 1 , V 2 , or V 6 discussed
V
previously favor the diagnosis of VT (Fig. 16-28).
Lead V : rsR' pattern Aberration
1
Lead V 6 or MCL 6 can be useful in differentiating supraven-
tricular rhythms with aberrancy from ventricular ectopy. 96,97 In
wide QRS rhythms of either RBBB or LBBB pattern, an inter- Lead V : R or qR with Ventricular
1
val of 50 milliseconds (0.05 second) or less from the onset of the taller LEFT rabbit ear
QRS to the tallest peak of the r wave or nadir of the S wave
favors a supraventricular origin, whereas an interval of 70
6
milliseconds (0.07 second) or more favors a ventricular origin Lead V : qRs Aberration
(Fig. 16-29).
Fusion and Capture Beats. Ventricular fusion beats are pro-
duced when a supraventricular impulse and an ectopic ventricular Lead V : QS or rS Ventricular
6
impulse both contribute to ventricular depolarization. The result-
ing QRS complex does not look like a normally conducted beat
or like the pure ventricular ectopic beat because it is formed by a
LBBB Morphology
In Leads V 1 or V 2 :
Wider wave ( .03 sec)
V1
Slurred downstroke Ventricular
.06 sec to nadir of S wave
A A
In Leads V1 or V2:
V1 Narrow r wave ( .03 sec)
Straight downstroke Aberration
.06 sec to nadir of S wave
B B
In Leads V :
6
■ Figure 16-25 Two similar wide QRS tachycardias. (A) Sinus Any q (QS or qR) Ventricular
tachycardia; rate—115 beats per minute. P waves can be seen preced-
ing each QRS, indicating a supraventricular origin of the tachycardia.
(B) P waves are independent of QRS complexes, indicating AV dis- ■ Figure 16-26 Morphology clues for wide QRS beats and
sociation that favors VT. rhythms with RBBB morphology and LBBB morphology.