
Page 406 - Cardiac Nursing
P. 406
xd
q
q
xd
6
6
Pa
q
Pa
33
33
3-3
87.
87.
3-3
/09
/09
2:1
/09
1
1
1
2:1
Pa
/30
/30
M
6 A
6 A
M
g
In
In
c.
a
ara
ara
a
LWBK340-c16_
LWB
LWB K34 0-c 16_ p p pp333-387.qxd 6/30/09 12:16 AM Page 382 Aptara Inc.
K34
c.
16_
0-c
t
e 3
82
82
g
g
e 3
82
p
p
t
p
A
A
382 P A R T III / Assessment of Heart Disease
V 1 1
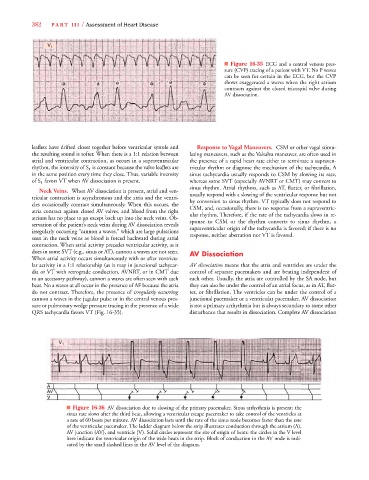
■ Figure 16-35 ECG and a central venous pres-
sure (CVP) tracing of a patient with VT. No P waves
can be seen for certain in the ECG, but the CVP
shows exaggerated a waves when the right atrium
contracts against the closed tricuspid valve during
AV dissociation.
leaflets have drifted closer together before ventricular systole and Response to Vagal Maneuvers. CSM or other vagal stimu-
the resulting sound is softer. When there is a 1:1 relation between lating maneuvers, such as the Valsalva maneuver, are often used in
atrial and ventricular contraction, as occurs in a supraventricular the presence of a rapid heart rate either to terminate a supraven-
rhythm, the intensity of S 1 is constant because the valve leaflets are tricular rhythm or diagnose the mechanism of the tachycardia. A
in the same position every time they close. Thus, variable intensity sinus tachycardia usually responds to CSM by slowing its rate,
of S 1 favors VT when AV dissociation is present. whereas some SVT (especially AVNRT or CMT) may convert to
sinus rhythm. Atrial rhythms, such as AT, flutter, or fibrillation,
Neck Veins. When AV dissociation is present, atrial and ven-
usually respond with a slowing of the ventricular response but not
tricular contraction is asynchronous and the atria and the ventri-
by conversion to sinus rhythm. VT typically does not respond to
cles occasionally contract simultaneously. When this occurs, the
CSM, and, occasionally, there is no response from a supraventric-
atria contract against closed AV valves, and blood from the right
ular rhythm. Therefore, if the rate of the tachycardia slows in re-
atrium has no place to go except back up into the neck veins. Ob-
sponse to CSM or the rhythm converts to sinus rhythm, a
servation of the patient’s neck veins during AV dissociation reveals
supraventricular origin of the tachycardia is favored; if there is no
irregularly occurring “cannon a waves,” which are large pulsations
response, neither aberration nor VT is favored.
seen in the neck veins as blood is forced backward during atrial
contraction. When atrial activity precedes ventricular activity, as it
does in some SVT (e.g., sinus or AT), cannon a waves are not seen. AV Dissociation
When atrial activity occurs simultaneously with or after ventricu-
lar activity in a 1:1 relationship (as it may in junctional tachycar- AV dissociation means that the atria and ventricles are under the
dia or VT with retrograde conduction, AVNRT, or in CMT due control of separate pacemakers and are beating independent of
to an accessory pathway), cannon a waves are often seen with each each other. Usually, the atria are controlled by the SA node, but
beat. No a waves at all occur in the presence of AF because the atria they can also be under the control of an atrial focus, as in AT, flut-
do not contract. Therefore, the presence of irregularly occurring ter, or fibrillation. The ventricles can be under the control of a
cannon a waves in the jugular pulse or in the central venous pres- junctional pacemaker or a ventricular pacemaker. AV dissociation
sure or pulmonary wedge pressure tracing in the presence of a wide is not a primary arrhythmia but is always secondary to some other
QRS tachycardia favors VT (Fig. 16-35). disturbance that results in dissociation. Complete AV dissociation
V 1 1
■ Figure 16-36 AV dissociation due to slowing of the primary pacemaker. Sinus arrhythmia is present; the
sinus rate slows after the third beat, allowing a ventricular escape pacemaker to take control of the ventricles at
a rate of 60 beats per minute. AV dissociation lasts until the rate of the sinus node becomes faster than the rate
of the ventricular pacemaker. The ladder diagram below the strip illustrates conduction through the atrium (A),
AV junction (AV), and ventricle (V). Solid circles represent the site of origin of beats: the circles in the V level
here indicate the ventricular origin of the wide beats in the strip. Block of conduction in the AV node is indi-
cated by the small slashed lines in the AV level of the diagram.