
Page 404 - Cardiac Nursing
P. 404
M
M
6 A
2:1
6 A
g
g
g
Pa
Pa
2:1
6
/30
6
xd
6
1
1
/09
/30
/09
a
a
ara
t
ara
c.
c.
c.
In
In
t
80
A
80
e 3
e 3
p
p
p
A
A
33
LWBK340-c16_ p p pp333-387.qxd 6/30/09 12:16 AM Page 380 Aptara Inc.
33
3-3
3-3
K34
16_
16_
0-c
K34
0-c
q
87.
87.
q
xd
q
380 P A R T III / Assessment of Heart Disease
V V V 1 1 1
A A
V 1
B B
V 1
C C
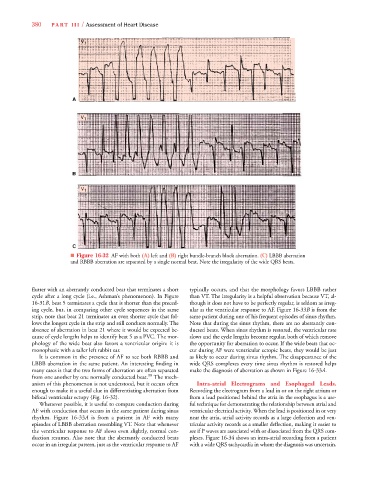
■ Figure 16-32 AF with both (A) left and (B) right bundle-branch block aberration. (C) LBBB aberration
and RBBB aberration are separated by a single normal beat. Note the irregularity of the wide QRS beats.
flutter with an aberrantly conducted beat that terminates a short typically occurs, and that the morphology favors LBBB rather
cycle after a long cycle (i.e., Ashman’s phenomenon). In Figure than VT. The irregularity is a helpful observation because VT, al-
16-31B, beat 5 terminates a cycle that is shorter than the preced- though it does not have to be perfectly regular, is seldom as irreg-
ing cycle, but, in comparing other cycle sequences in the same ular as the ventricular response to AF. Figure 16-33B is from the
strip, note that beat 21 terminates an even shorter cycle that fol- same patient during one of his frequent episodes of sinus rhythm.
lows the longest cycle in the strip and still conducts normally. The Note that during the sinus rhythm, there are no aberrantly con-
absence of aberration in beat 21 where it would be expected be- ducted beats. When sinus rhythm is restored, the ventricular rate
cause of cycle lengths helps to identify beat 5 as a PVC. The mor- slows and the cycle lengths become regular, both of which remove
phology of the wide beat also favors a ventricular origin: it is the opportunity for aberration to occur. If the wide beats that oc-
monophasic with a taller left rabbit ear. cur during AF were ventricular ectopic beats, they would be just
It is common in the presence of AF to see both RBBB and as likely to occur during sinus rhythm. The disappearance of the
LBBB aberration in the same patient. An interesting finding in wide QRS complexes every time sinus rhythm is restored helps
3
3
many cases is that the two forms of aberration are often separated make the diagnosis of aberration as shown in Figure 16-33A.
99
from one another by one normally conducted beat. The mech-
anism of this phenomenon is not understood, but it occurs often Intra-atrial Electrograms and Esophageal Leads.
enough to make it a useful clue in differentiating aberration from Recording the electrogram from a lead in or on the right atrium or
bifocal ventricular ectopy (Fig. 16-32). from a lead positioned behind the atria in the esophagus is a use-
Whenever possible, it is useful to compare conduction during ful technique for demonstrating the relationship between atrial and
AF with conduction that occurs in the same patient during sinus ventricular electrical activity. When the lead is positioned in or very
rhythm. Figure 16-33A is from a patient in AF with many near the atria, atrial activity records as a large deflection and ven-
episodes of LBBB aberration resembling VT. Note that whenever tricular activity records as a smaller deflection, making it easier to
the ventricular response to AF slows even slightly, normal con- see if P waves are associated with or dissociated from the QRS com-
duction resumes. Also note that the aberrantly conducted beats plexes. Figure 16-34 shows an intra-atrial recording from a patient
occur in an irregular pattern, just as the ventricular response to AF with a wide QRS tachycardia in whom the diagnosis was uncertain.