
Page 403 - Cardiac Nursing
P. 403
2:1
6 A
2:1
1
1
6 A
Pa
Pa
Pa
M
M
1
xd
6
xd
q
q
6
/09
/09
/09
/30
/30
ara
ara
t
p
t
a
c.
c.
In
a
In
p
e 3
e 3
g
g
g
79
A
p
A
79
79
q
K34
K34
LWB
LWB
p
16_
0-c
0-c
LWBK340-c16_ p pp333-387.qxd 6/30/09 12:16 AM Page 379 Aptara Inc.
16_
3-3
87.
87.
33
33
3-3
C HAPTER 1 6 / Arrhythmias and Conduction Disturbances 379
V 1
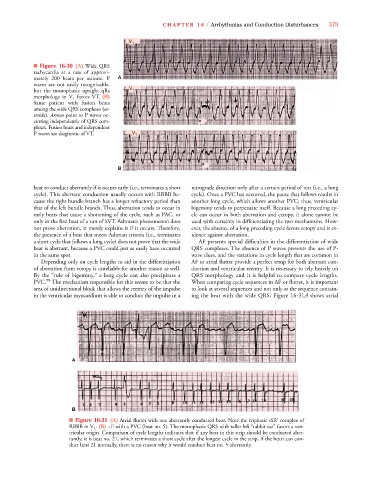
■ Figure 16-30 (A) Wide QRS
tachycardia at a rate of approxi-
mately 200 beats per minute. P A
waves are not easily recognizable,
but the monophasic upright qRs V 1
morphology in V 1 favors VT. (B)
Same patient with fusion beats
among the wide QRS complexes (as-
terisks). Arrows point to P waves oc-
s
curring independently of QRS com-
plexes. Fusion beats and independent
P waves are diagnostic of VT. V 1
B
beat to conduct aberrantly if it occurs early (i.e., terminates a short retrograde direction only after a certain period of rest (i.e., a long
cycle). This aberrant conduction usually occurs with RBBB be- cycle). Once a PVC has occurred, the pause that follows results in
cause the right bundle branch has a longer refractory period than another long cycle, which allows another PVC; thus, ventricular
that of the left bundle branch. Thus, aberration tends to occur in bigeminy tends to perpetuate itself. Because a long preceding cy-
early beats that cause a shortening of the cycle, such as PAC, or cle can occur in both aberration and ectopy, it alone cannot be
only in the first beat of a run of SVT. Ashman’s phenomenon does used with certainty in differentiating the two mechanisms. How-
not prove aberration, it merely explains it if it occurs. Therefore, ever, the absence of a long preceding cycle favors ectopy and is ev-
the presence of a beat that meets Ashman criteria (i.e., terminates idence against aberration.
a short cycle that follows a long cycle) does not prove that the wide AF presents special difficulties in the differentiation of wide
beat is aberrant, because a PVC could just as easily have occurred QRS complexes. The absence of P waves prevents the use of P-
in the same spot. wave clues, and the variations in cycle length that are common in
Depending only on cycle lengths to aid in the differentiation AF or atrial flutter provide a perfect setup for both aberrant con-
of aberration from ectopy is unreliable for another reason as well. duction and ventricular reentry. It is necessary to rely heavily on
By the “rule of bigeminy,” a long cycle can also precipitate a QRS morphology and it is helpful to compare cycle lengths.
PVC. 98 The mechanism responsible for this seems to be that the When comparing cycle sequences in AF or flutter, it is important
area of unidirectional block that allows the reentry of the impulse to look at several sequences and not only at the sequence contain-
in the ventricular myocardium is able to conduct the impulse in a ing the beat with the wide QRS. Figure 16-31A shows atrial
A A
B
■ Figure 16-31 (A) Atrial flutter with one aberrantly conducted beat. Note the triphasic rSR’ complex of
RBBB in V 1 . (B) AF with a PVC (beat no. 5). The monophasic QRS with taller left “rabbit ear” favors a ven-
tricular origin. Comparison of cycle lengths indicates that if any beat in this strip should be conducted aber-
rantly, it is beat no. 21, which terminates a short cycle after the longest cycle in the strip. If the heart can con-
duct beat 21 normally, there is no reason why it would conduct beat no. 5 aberrantly.