
Page 469 - Cardiac Nursing
P. 469
Pa
Pa
M
9 P
M
g
e 4
g
Pa
g
/09
1
/09
/29
/09
1:2
9 P
1:2
1
1
a
a
a
ara
ara
c.
c.
In
a
In
A
A
45
e 4
45
t
t
p
p
p
9-4
9-4
xd
6
xd
59.
q
q
q
59.
59.
6
LWBK340-c20_
K34
LWB
/29
LWB K34 0-c 20_ p p pp439-459.qxd 6/29/09 11:29 PM Page 445 Aptara Inc.
43
43
20_
0-c
20_
C HAPTER 2 0 / Cardiac Catheterization 445
Brachial
insertion
site
Radial
insertion
site
ANTERIOR
SPINE
Femoral
insertion INGUINAL
site LIGAMENT
SKIN
CREASE
c
c
c
c
cm
m
m
m
m
m
cm
cm
cm
cm
cm
cm
c
c
c
c
c
m
m
m
m
m
m
m
m
m
m
m
m
m
m
m
m
m
m
m
m
m
m
cm
3 c
3 c
3 cm
3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 c
3 c
3 c cm
3 c
3 c
cm
c
cm
cm
3 c
3 c
c
3 c
X X X X X X X X X X X X X
COMMON
FEMORAL
ARTERY
PROFUNDA
SAPHENOUS
VEIN
SUPERFICIAL
FEMORAL ARTERY FEMORAL
A B VEIN
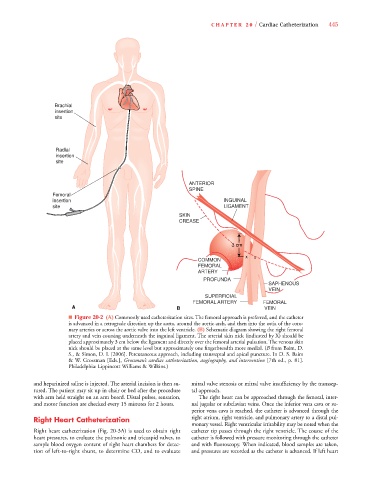
■ Figure 20-2 (A) Commonly used catheterization sites. The femoral approach is preferred, and the catheter
is advanced in a retrograde direction up the aorta, around the aortic arch, and then into the ostia of the coro-
nary arteries or across the aortic valve into the left ventricle. (B) Schematic diagram showing the right femoral
artery and vein coursing underneath the inguinal ligament. The arterial skin nick (indicated by X) should be
placed approximately 3 cm below the ligament and directly over the femoral arterial pulsation. The venous skin
nick should be placed at the same level but approximately one fingerbreadth more medial. (B from Baim, D.
S., & Simon, D. I. [2006]. Percutaneous approach, including transseptal and apical puncture. In D. S. Baim
& W. Grossman [Eds.], Grossman’s cardiac catheterization, angiography, and intervention [7th ed., p. 81].
Philadelphia: Lippincott Williams & Wilkins.)
and heparinized saline is injected. The arterial incision is then su- mitral valve stenosis or mitral valve insufficiency by the transsep-
tured. The patient may sit up in chair or bed after the procedure tal approach.
with arm held straight on an arm board. Distal pulses, sensation, The right heart can be approached through the femoral, inter-
and motor function are checked every 15 minutes for 2 hours. nal jugular or subclavian veins. Once the inferior vena cava or su-
perior vena cava is reached, the catheter is advanced through the
Right Heart Catheterization right atrium, right ventricle, and pulmonary artery to a distal pul-
monary vessel. Right ventricular irritability may be noted when the
Right heart catheterization (Fig. 20-3A) is used to obtain right catheter tip passes through the right ventricle. The course of the
heart pressures, to evaluate the pulmonic and tricuspid valves, to catheter is followed with pressure monitoring through the catheter
sample blood oxygen content of right heart chambers for detec- and with fluoroscopy. When indicated, blood samples are taken,
tion of left-to-right shunt, to determine CO, and to evaluate and pressures are recorded as the catheter is advanced. If left heart