
Page 470 - Cardiac Nursing
P. 470
/09
1
1
/29
/09
/09
1
9 P
M
M
1:2
1:2
9 P
59.
59.
q
9-4
9-4
59.
q
6
6
/29
q
xd
xd
Pa
ara
ara
a
p
t
t
a
In
c.
c.
a
a
In
g
g
e 4
Pa
Pa
g
e 4
A
p
p
46
46
A
K34
K34
LWB
LWBK340-c20_ p p pp439-459.qxd 6/29/09 11:29 PM Page 446 Aptara Inc.
LWB
20_
20_
20_
0-c
0-c
43
43
446 P A R T III / Assessment of Heart Disease
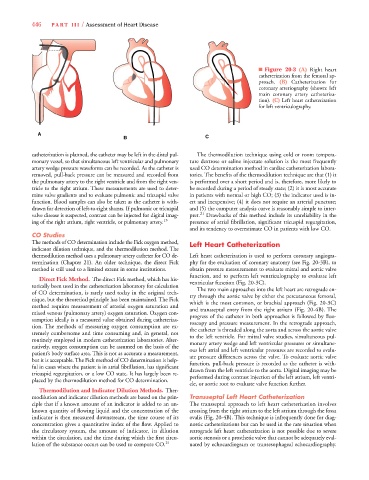
■ Figure 20-3 (A) Right heart
catheterization from the femoral ap-
proach. (B) Catheterization for
coronary arteriography (shown: left
main coronary artery catheteriza-
tion). (C) Left heart catheterization
for left ventriculography.
A
B C
catheterization is planned, the catheter may be left in the distal pul- The thermodilution technique using cold or room tempera-
monary vessel, so that simultaneous left ventricular and pulmonary ture dextrose or saline injectate solution is the most frequently
artery wedge pressure waveforms can be recorded. As the catheter is used CO determination method in cardiac catheterization labora-
removed, pull-back pressure can be measured and recorded from tories. The benefits of the thermodilution technique are that (1) it
the pulmonary artery to the right ventricle and from the right ven- is performed over a short period and is, therefore, more likely to
tricle to the right atrium. These measurements are used to deter- be recorded during a period of steady state; (2) it is most accurate
mine valve gradients and to evaluate pulmonic and tricuspid valve in patients with normal or high CO; (3) the indicator used is in-
function. Blood samples can also be taken as the catheter is with- ert and inexpensive; (4) it does not require an arterial puncture;
drawn for detection of left-to-right shunts. If pulmonic or tricuspid and (5) the computer analysis curve is reasonably simple to inter-
valve disease is suspected, contrast can be injected for digital imag- pret. 21 Drawbacks of this method include its unreliability in the
ing of the right atrium, right ventricle, or pulmonary artery. 13 presence of atrial fibrillation, significant tricuspid regurgitation,
and its tendency to overestimate CO in patients with low CO.
CO Studies
The methods of CO determination include the Fick oxygen method, Left Heart Catheterization
indicator dilution technique, and the thermodilution method. The
thermodilution method uses a pulmonary artery catheter for CO de- Left heart catheterization is used to perform coronary angiogra-
termination (Chapter 21). An older technique, the direct Fick phy for the evaluation of coronary anatomy (see Fig. 20-3B), to
method is still used to a limited extent in some institutions. obtain pressure measurements to evaluate mitral and aortic valve
function, and to perform left ventriculography to evaluate left
Direct Fick Method. The direct Fick method, which has his-
ventricular function (Fig. 20-3C).
torically been used in the catheterization laboratory for calculation
The two main approaches into the left heart are retrograde en-
of CO determination, is rarely used today in the original tech-
try through the aortic valve by either the percutaneous femoral,
nique, but the theoretical principle has been maintained. The Fick
which is the most common, or brachial approach (Fig. 20-3C)
method requires measurement of arterial oxygen saturation and
and transseptal entry from the right atrium (Fig. 20-4B). The
mixed venous (pulmonary artery) oxygen saturation. Oxygen con-
progress of the catheter in both approaches is followed by fluo-
sumption ideally is a measured value obtained during catheteriza-
roscopy and pressure measurement. In the retrograde approach,
tion. The methods of measuring oxygen consumption are ex-
the catheter is threaded along the aorta and across the aortic valve
tremely cumbersome and time consuming and, in general, not
to the left ventricle. For mitral valve studies, simultaneous pul-
routinely employed in modern catheterization laboratories. Alter-
monary artery wedge and left ventricular pressures or simultane-
natively, oxygen consumption can be assumed on the basis of the
ous left atrial and left ventricular pressures are recorded to evalu-
patient’s body surface area. This is not as accurate a measurement,
ate pressure differences across the valve. To evaluate aortic valve
but it is acceptable. The Fick method of CO determination is help-
function, pull-back pressure is recorded as the catheter is with-
ful in cases where the patient is in atrial fibrillation, has significant
drawn from the left ventricle to the aorta. Digital imaging may be
tricuspid regurgitation, or a low CO state. It has largely been re-
performed during contrast injection of the left atrium, left ventri-
placed by the thermodilution method for CO determination.
cle, or aortic root to evaluate valve function further.
Thermodilution and Indicator Dilution Methods. Ther-
modilution and indicator dilution methods are based on the prin- Transseptal Left Heart Catheterization
ciple that if a known amount of an indicator is added to an un- The transseptal approach to left heart catheterization involves
known quantity of flowing liquid and the concentration of the crossing from the right atrium to the left atrium through the fossa
indicator is then measured downstream, the time course of its ovalis (Fig. 20-4B). This technique is infrequently done for diag-
concentration gives a quantitative index of the flow. Applied to nostic catheterizations but can be used in the rare situation when
the circulatory system, the amount of indicator, its dilution retrograde left heart catheterization is not possible due to severe
within the circulation, and the time during which the first circu- aortic stenosis or a prosthetic valve that cannot be adequately eval-
lation of the substance occurs can be used to compute CO. 21 uated by echocardiogram or transesophageal echocardiography.