
Page 472 - Cardiac Nursing
P. 472
/09
1
/09
/09
1:2
1:2
1
1
In
/29
p
6
/29
c.
c.
In
a
e 4
48
g
e 4
A
p
48
A
g
M
M
9 P
9 P
Pa
g
Pa
Pa
a
a
20_
a
t
t
ara
ara
20_
LWB
K34
LWBK340-c20_ pp439-459.qxd 6/29/09 11:29 PM Page 448 Aptara Inc.
LWB
0-c
20_
K34
0-c
q
q
59.
59.
xd
6
q
xd
59.
p
43
p
p
9-4
9-4
43
448 P A R T III / Assessment of Heart Disease
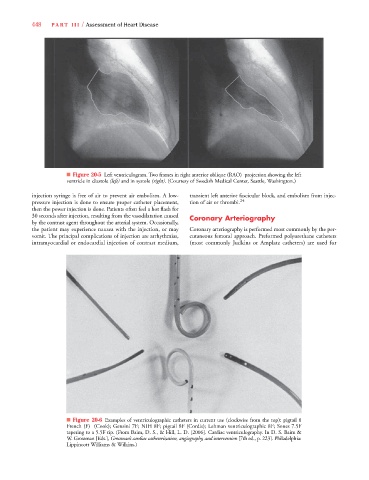
■ Figure 20-5 Left ventriculogram. Two frames in right anterior oblique (RAO) projection showing the left
ventricle in diastole (left) and in systole (right). (Courtesy of Swedish Medical Center, Seattle, Washington.)
injection syringe is free of air to prevent air embolism. A low- transient left anterior fascicular block, and embolism from injec-
pressure injection is done to ensure proper catheter placement, tion of air or thrombi. 24
then the power injection is done. Patients often feel a hot flash for
30 seconds after injection, resulting from the vasodilatation caused Coronary Arteriography
by the contrast agent throughout the arterial system. Occasionally,
the patient may experience nausea with the injection, or may Coronary arteriography is performed most commonly by the per-
vomit. The principal complications of injection are arrhythmias, cutaneous femoral approach. Preformed polyurethane catheters
intramyocardial or endocardial injection of contrast medium, (most commonly Judkins or Amplatz catheters) are used for
■ Figure 20-6 Examples of ventriculographic catheters in current use (clockwise from the top): pigtail 8
French (F) (Cook); Gensini 7F; NIH 8F; pigtail 8F (Cordis); Lehman ventriculographic 8F; Sones 7.5F
tapering to a 5.5F tip. (From Baim, D. S., & Hill, L. D. [2006]. Cardiac ventriculography. In D. S. Baim &
W. Grossman [Eds.], Grossman’s cardiac catheterization, angiography, and intervention [7th ed., p. 223]. Philadelphia:
Lippincott Williams & Wilkins.)