
Page 471 - Cardiac Nursing
P. 471
9 P
9 P
1:2
1
1:2
M
Pa
g
Pa
M
Pa
1
6
6
xd
q
xd
/29
/09
1
/09
/29
/09
a
a
ara
t
ara
a
c.
c.
In
a
In
t
e 4
47
e 4
g
g
47
p
p
p
A
A
q
LWB K34 0-c 20_ p p pp439-459.qxd 6/29/09 11:29 PM Page 447 Aptara Inc.
LWB
43
43
LWBK340-c20_
20_
20_
K34
0-c
59.
9-4
9-4
q
59.
59.
C HAPTER 2 0 / Cardiac Catheterization 447
A B B
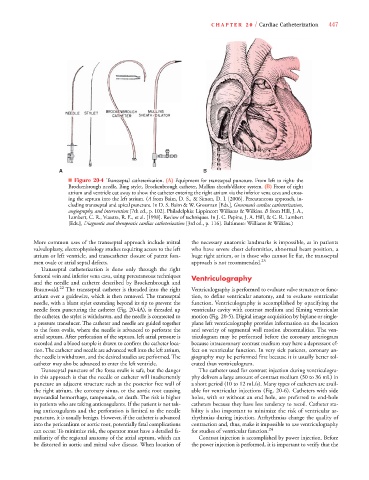
■ Figure 20-4 Transseptal catheterization. (A) Equipment for transseptal puncture. From left to right: the
Brockenbrough needle, Bing stylet, Brockenbrough catheter, Mullins sheath/dilator system. (B) Front of right
atrium and ventricle cut away to show the catheter entering the right atrium via the inferior vena cava and cross-
ing the septum into the left atrium. (A from Baim, D. S., & Simon, D. I. [2006]. Percutaneous approach, in-
(
(
cluding transseptal and apical puncture. In D. S. Baim & W. Grossman [Eds.], Grossman’s cardiac catheterization,
angiography, and intervention [7th ed., p. 102]. Philadelphia: Lippincott Williams & Wilkins. B from Hill, J. A.,
Lambert, C. R., Vuestra, R. E., et al. [1998]. Review of techniques. In J. C. Pepine, J. A. Hill, & C. R. Lambert
[Eds.], Diagnostic and therapeutic cardiac catheterization [3rd ed., p. 116]. Baltimore: Williams & Wilkins.)
More common uses of the transseptal approach include mitral the necessary anatomic landmarks is impossible, as in patients
valvuloplasty, electrophysiology studies requiring access to the left who have severe chest deformities, abnormal heart position, a
atrium or left ventricle, and transcatheter closure of patent fora- huge right atrium, or in those who cannot lie flat, the transseptal
men ovale or atrial septal defects. approach is not recommended. 23
Transseptal catheterization is done only through the right
femoral vein and inferior vena cava, using percutaneous techniques Ventriculography
and the needle and catheter described by Brockenbrough and
Braunwald. 22 The transseptal catheter is threaded into the right Ventriculography is performed to evaluate valve structure or func-
atrium over a guidewire, which is then removed. The transseptal tion, to define ventricular anatomy, and to evaluate ventricular
needle, with a blunt stylet extending beyond its tip to prevent the function. Ventriculography is accomplished by opacifying the
needle from puncturing the catheter (Fig. 20-4A), is threaded up ventricular cavity with contrast medium and filming ventricular
the catheter, the stylet is withdrawn, and the needle is connected to motion (Fig. 20-5). Digital image acquisition by biplane or single-
a pressure transducer. The catheter and needle are guided together plane left ventriculography provides information on the location
to the fossa ovalis, where the needle is advanced to perforate the and severity of segmental wall motion abnormalities. The ven-
atrial septum. After perforation of the septum, left atrial pressure is triculogram may be performed before the coronary arteriogram
recorded and a blood sample is drawn to confirm the catheter loca- because intracoronary contrast medium may have a depressant ef-
tion. The catheter and needle are advanced well into the left atrium, fect on ventricular function. In very sick patients, coronary an-
the needle is withdrawn, and the desired studies are performed. The giography may be performed first because it is usually better tol-
catheter may also be advanced to enter the left ventricle. erated than ventriculogram.
Transseptal puncture of the fossa ovalis is safe, but the danger The catheter used for contrast injection during ventriculogra-
in this approach is that the needle or catheter will inadvertently phy delivers a large amount of contrast medium (30 to 36 mL) in
puncture an adjacent structure such as the posterior free wall of a short period (10 to 12 mL/s). Many types of catheters are avail-
the right atrium, the coronary sinus, or the aortic root causing able for ventricular injections (Fig. 20-6). Catheters with side
myocardial hemorrhage, tamponade, or death. The risk is higher holes, with or without an end hole, are preferred to end-hole
in patients who are taking anticoagulants. If the patient is not tak- catheters because they have less tendency to recoil. Catheter sta-
ing anticoagulants and the perforation is limited to the needle bility is also important to minimize the risk of ventricular ar-
puncture, it is usually benign. However, if the catheter is advanced rhythmias during injection. Arrhythmias change the quality of
into the pericardium or aortic root, potentially fatal complications contraction and, thus, make it impossible to use ventriculography
can occur. To minimize risk, the operator must have a detailed fa- for studies of ventricular function. 24
miliarity of the regional anatomy of the atrial septum, which can Contrast injection is accomplished by power injection. Before
be distorted in aortic and mitral valve disease. When location of the power injection is performed, it is important to verify that the