
Page 605 - Cardiac Nursing
P. 605
0
0
009
009
1:4
3 P
M
1:4
3 P
3
3
xd
xd
3
6/2
6/2
0/0
0/0
M
p
p
A
A
p
ara
ara
t
t
g
g
Pa
Pa
g
81
81
e 5
e 5
q
55
55
LWB K34 0-c 24_ p p pp555-594.qxd 30/06/2009 01:43 PM Page 581 Aptara
LWBK340-c24_
0-c
24_
LWB
K34
94.
q
q
94.
5-5
5-5
C HAPTER 24 / Heart Failure and Cardiogenic Shock 581
stimulation, hormones are released from the adrenal medulla, ad- no longer able to maintain homeostasis and may become coun-
renal cortex, anterior and posterior pituitary gland, and kidneys, terproductive. For example, continued profound vasoconstriction
which further compensate for decreased circulating blood volume. in the presence of decreased MAP promotes inadequate tissue per-
The adrenal medulla releases epinephrine and NE, which enhance fusion and cellular hypoxia.
vasoconstriction and myocardial contractility, and increase heart Decreased delivery of oxygen and nutrients causes cells to
13
7
rate. Epinephrine and NE also stimulate glycogenolysis, thus in- shift to anaerobic metabolic pathways. Increasing amounts of
creasing serum glucose. The adrenal cortex releases glucocorticoids, lactic acid are produced and accumulate in the cells because of
which also increase serum glucose. Decreased renal blood flow re- decreased perfusion. Because anaerobic metabolism is less effi-
sults in the release of renin, which initiates a series of reactions in cient in meeting the energy requirements of the cells, ATP is
the liver and elsewhere, resulting in the production of angiotensin. depleted. Reduction in the available ATP results in failure of
Angiotensin promotes the release of aldosterone by the adrenal cor- the membrane transport mechanisms, intracellular edema, and
tex and, in situations of hypovolemia, promotes profound vaso- rupture of the cell membrane. Progressive tissue ischemia results
constriction. Aldosterone enhances renal sodium reabsorption ac- in increased anaerobic metabolism and the further production of
companied by increased water reabsorption. Antidiuretic hormone metabolic acidosis. 190
is released from the posterior pituitary and further enhances renal Impairment of cellular function disrupts all body organs and
water reabsorption. Thirst is stimulated and also causes increased organ systems. Splanchnic ischemia results in the release of endo-
fluid intake. 11 As a result of decreased capillary pressure, Starling toxin from the intestine. The reticuloendothelial (tissue
capillary forces are altered, and fluid is transferred from the inter- macrophage) system is suppressed by splenic and hepatic is-
stitial space to the capillary. chemia. The continued renal response to ischemia leads to fur-
ther vasoconstriction, stimulating the release of aldosterone
Intermediate Stage from the adrenal gland and promoting the reabsorption of
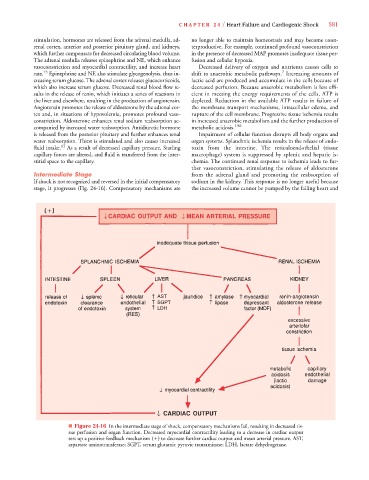
If shock is not recognized and reversed in the initial compensatory sodium in the kidney. This response is no longer useful because
stage, it progresses (Fig. 24-16). Compensatory mechanisms are the increased volume cannot be pumped by the failing heart and
AST
SGPT
LDH
■ Figure 24-16 In the intermediate stage of shock, compensatory mechanisms fail, resulting in decreased tis-
sue perfusion and organ function. Decreased myocardial contractility leading to a decrease in cardiac output
sets up a positive feedback mechanism (
) to decrease further cardiac output and mean arterial pressure. AST,
aspartate aminotransferase; SGPT, serum glutamic pyruvic transaminase; LDH, lactate dehydrogenase.