
Page 76 - Cardiac Nursing
P. 76
3
3
5:3
Pa
Pa
Pa
5:3
009
0/2
0/2
1
1
009
g
ta
p
p
r
r
ta
p
e 5
g
g
2 A
2 A
e 5
6/3
68.
q
2-0
68.
xd
xd
q
q
2-0
LWBK340-c02_
K34
LWB K34 0-c 02_ p p pp042-068.qxd 06/30/2009 15:33 Page 52 Aptara a a
LWB
04
04
0-c
02_
0
6/3
0
0
52 PA R T I / Anatomy and Physiology
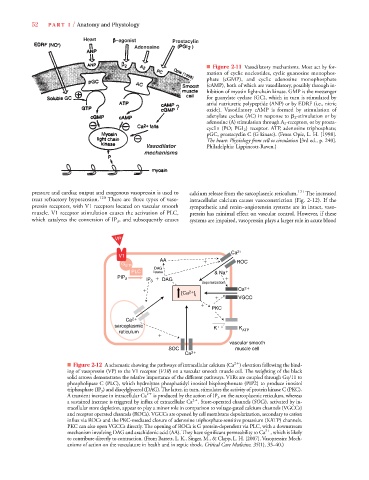
■ Figure 2-11 Vasodilatory mechanisms. Most act by for-
mation of cyclic nucleotides, cyclic guanosine monophos-
phate (cGMP), and cyclic adenosine monophosphate
(cAMP), both of which are vasodilatory, possibly through in-
hibition of myosin light-chain kinase. GMP is the messenger
for guanylate cyclase (GC), which in turn is stimulated by
atrial natriuretic polypeptide (ANP) or by EDRF (i.e., nitric
oxide). Vasodilatory cAMP is formed by stimulation of
adenylate cyclase (AC) in response to 2 -stimulation or by
adenosine (A) stimulation through A 2 -receptors, or by prosta-
A
cyclin (PO; PGI 2 ) receptor. ATP, adenosine triphosphate;
pGC, prostacyclin C (G kinase). (From Opie, L. H. [1998].
The heart: Physiology from cell to circulation [3rd ed., p. 240].
Philadelphia: Lippincott-Raven.)
pressure and cardiac output and exogenous vasopressin is used to calcium release from the sarcoplasmic reticulum. 121 The increased
treat refractory hypotension. 120 There are three types of vaso- intracellular calcium causes vasoconstriction (Fig. 2-12). If the
pressin receptors, with V1 receptors located on vascular smooth sympathetic and renin–angiotensin systems are in intact, vaso-
muscle. V1 receptor stimulation causes the activation of PLC, pressin has minimal effect on vascular control. However, if these
which catalyzes the conversion of IP 3 , and subsequently causes systems are impaired, vasopressin plays a larger role in acute blood
VP
Ca 2
V1
AA
ROC
G q/11
DAG
PLC lipase & Na
PIP 2 IP
DAG
3
depolarization
2
Ca 2
[Ca ]
i
VGCC
PKC
Ca 2
sarcoplasmic K
K
reticulum ATP
vascular smooth
SOC muscle cell
Ca 2
2
■ Figure 2-12 A schematic showing the pathways of intracellular calcium (Ca ) elevation following the bind-
ing of vasopressin (VP) to the V1 receptor (V1R) on a vascular smooth muscle cell. The weighting of the black
R
R
solid arrows demonstrates the relative importance of the different pathways. V1Rs are coupled through Gq/11 to
phospholipase C (PLC), which hydrolyzes phosphatidyl inositol bisphosphonate (PIP2) to produce inositol
triphosphate (IP 3 ) and diacylglycerol (DAG). The latter, in turn, stimulates the activity of protein kinase C (PKC).
A transient increase in intracellular Ca 2
is produced by the action of IP 3 on the sarcoplasmic reticulum, whereas
2
a sustained increase is triggered by influx of extracellular Ca . Store-operated channels (SOCs), activated by in-s
tracellular store depletion, appear to play a minor role in comparison to voltage-gated calcium channels (VGCCs)
and receptor operated channels (ROCs). VGCCs are opened by cell membrane depolarization, secondary to cation
influx via ROCs and the PKC-mediated closure of adenosine triphosphate-sensitive potassium (KATP) channels.
PKC can also open VGCCs directly. The opening of ROCs is G protein-dependent via PLC, with a downstream
2
mechanism involving DAG and arachidonic acid (AA). They have significant permeability to Ca , which is likely
to contribute directly to contraction. (From Barrett, L. K., Singer, M., & Clapp, L. H. [2007]. Vasopressin: Mech-
anisms of action on the vasculature in health and in septic shock. Critical Care Medicine, 35(1), 33–40.)