
Page 71 - Cardiac Nursing
P. 71
LWBK340-c02_p042-068.qxd 06/30/2009 15:33 Page 47 Aptara
C HAP TE R 2 / Systemic and Pulmonary Circulation and Oxygen Delivery 47
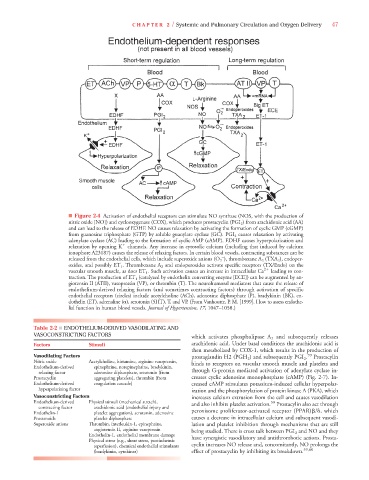
■ Figure 2-4 Activation of endothelial receptors can stimulate NO synthase (NOS, with the production of
nitric oxide [NO]) and cyclooxygenase (COX), which produces prostacyclin (PGI 2 ) from arachidonic acid (AA)
and can lead to the release of EDHF. NO causes relaxation by activating the formation of cyclic GMP (cGMP)
from guanosine triphosphate (GTP) by soluble guanylate cyclase (GC). PGI 2 causes relaxation by activating
adenylate cyclase (AC) leading to the formation of cyclic AMP (cAMP). EDHF causes hyperpolarization and
relaxation by opening K channels. Any increase in cytosolic calcium (including that induced by calcium
ionophore A23187) causes the release of relaxing factors. In certain blood vessels, contracting substances can be
–
released from the endothelial cells, which include superoxide anions (O 2 ), thromboxane A 2 (TXA 2 ), endoper-
A
oxides, and possibly ET 1 . Thromboxane A 2 and endoperoxides activate specific receptors (TX/Endo) on the
A
vascular smooth muscle, as does ET 1 . Such activation causes an increase in intracellular Ca 2
leading to con-
traction. The production of ET 1 (catalyzed by endothelin converting enzyme [ECE]) can be augmented by an-
giotensin II (ATII), vasopressin (VP), or thrombin (T). The neurohumoral mediators that cause the release of
endothelium-derived relaxing factors (and sometimes contracting factors) through activation of specific
endothelial receptors (circles) include acetylcholine (ACh), adenosine diphosphate (P), bradykinin (BK), en-
dothelin (ET), adrenaline ( ), serotonin (5HT), T, and VP. (From Vanhoutte, P. M. [1999]. How to assess endothe-
7
7
lial function in human blood vessels. Journal of Hypertension, 17, 1047–1058.)
Table 2-2 ■ ENDOTHELIUM-DERIVED VASODILATING AND
VASOCONSTRICTING FACTORS which activates phospholipase A 2 and subsequently releases
Factors Stimuli arachidonic acid. Under basal conditions the arachidonic acid is
then metabolized by COX-1, which results in the production of
Vasodilating Factors prostaglandin H2 (PGH 2 ) and subsequently PGI 2 . 59 Prostacylin
Nitric oxide Acetylcholine, histamine, arginine vasopressin, binds to receptors on vascular smooth muscle and platelets and
Endothelium-derived epinephrine, norepinephrine, bradykinin,
relaxing factor adenosine diphosphate, serotonin (from through G-protein mediated activation of adenylate cyclase in-
Prostacyclin aggregating platelets), thrombin (from creases cyclic adenosine monophosphate (cAMP) (Fig. 2-7). In-
Endothelium-derived coagulation cascade) creased cAMP stimulates potassium-induced cellular hyperpolar-
hyperpolarizing factor ization and the phosphorylation of protein kinase A (PKA), which
Vasoconstricting Factors increases calcium extrusion from the cell and causes vasodilation
Endothelium-derived Physical stimuli (mechanical stretch), and also inhibits platelet activation. Prostacylin also act through
59
contracting factor arachidonic acid (endothelial injury and
Endothelin-1 platelet aggregation), serotonin, adenosine peroxisome proliferator-activated receptor (PPAR) /
, which
Prostanoids platelet diphosphate causes a decrease in intracellular calcium and subsequent vasodi-
Superoxide anions Thrombin, interleukin-1, epinephrine, lation and platelet inhibition through mechanisms that are still
angiotensin II, arginine vasopressin being studied. There is cross talk between PGI 2 and NO and they
Endothelin-1, endothelial membrane damage
Physical stress (e.g., shear stress, postischemic have synergistic vasodilatory and antithrombotic actions. Prosta-
reperfusion), chemical endothelial stimulants cyclin increases NO release and, concomitantly, NO prolongs the
(bradykinin, cytokines) effect of prostacyclin by inhibiting its breakdown. 59,60