
Page 333 - ACCCN's Critical Care Nursing
P. 333
310 P R I N C I P L E S A N D P R A C T I C E O F C R I T I C A L C A R E
Left side battery
omitted for clarity
Aorta
Heart
External
battery
pack
A
XVE
LVAD
Skin
line
Vent adapter &
XVE System vent filter
B controller
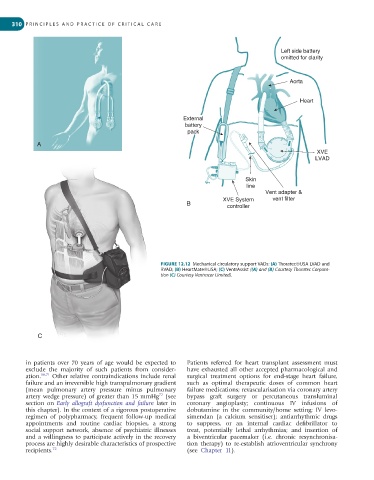
FIGURE 12.12 Mechanical circulatory support VADs: (A) Thoratec®USA LVAD and
RVAD; (B) HeartMate®USA; (C) VentrAssist ((A) and (B) Courtesy Thoratec Corpora-
tion (C) Courtesy Ventracor Limited).
C
in patients over 70 years of age would be expected to Patients referred for heart transplant assessment must
exclude the majority of such patients from consider- have exhausted all other accepted pharmacological and
ation. 66,71 Other relative contraindications include renal surgical treatment options for end-stage heart failure,
failure and an irreversible high transpulmonary gradient such as optimal therapeutic doses of common heart
(mean pulmonary artery pressure minus pulmonary failure medications; revascularisation via coronary artery
72
artery wedge pressure) of greater than 15 mmHg (see bypass graft surgery or percutaneous transluminal
section on Early allograft dysfunction and failure later in coronary angioplasty; continuous IV infusions of
this chapter). In the context of a rigorous postoperative do butamine in the community/home setting; IV levo-
regimen of polypharmacy, frequent follow-up medical simendan (a calcium sensitiser); antiarrhythmic drugs
appointments and routine cardiac biopsies, a strong to suppress, or an internal cardiac defibrillator to
social support network, absence of psychiatric illnesses treat, potentially lethal arrhythmias; and insertion of
and a willingness to participate actively in the recovery a biventri cular pacemaker (i.e. chronic resynchronisa-
process are highly desirable characteristics of prospective tion therapy) to re-establish atrioventricular synchrony
recipients. 72 (see Chapter 11).