
Page 516 - ACCCN's Critical Care Nursing
P. 516
Support of Renal Function 493
MAJOR CIRCUIT COMPONENTS FOR CRRT weight <20,000 daltons), while larger plasma proteins
65
To correctly use and ‘troubleshoot’ the various modes of and blood cells (at least 60–70,000 daltons) are retained.
RRT, nurses must have a clear understanding of the circuit Plasma water separated from the blood in this way is
components and their function. carried away from the filter by a side exit port and a pump,
where it is measured and directed into a collection bottle
Membranes or bag as waste; this convective clearance of solutes is
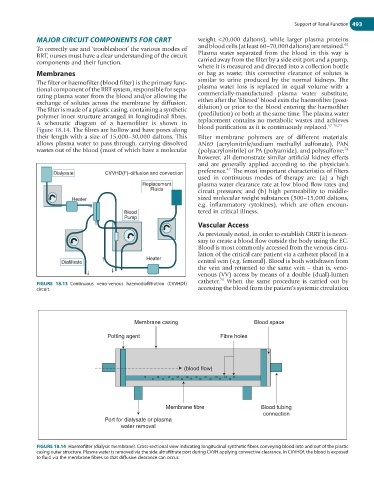
The filter or haemofilter (blood filter) is the primary func- similar to urine produced by the normal kidneys. The
tional component of the RRT system, responsible for sepa- plasma water loss is replaced in equal volume with a
rating plasma water from the blood and/or allowing the commercially-manufactured plasma water substitute,
exchange of solutes across the membrane by diffusion. either after the ‘filtered’ blood exits the haemofilter (post-
The filter is made of a plastic casing, containing a synthetic dilution) or prior to the blood entering the haemofilter
polymer inner structure arranged in longitudinal fibres. (predilution) or both at the same time. The plasma water
A schematic diagram of a haemofilter is shown in replacement contains no metabolic wastes and achieves
67-70,73
Figure 18.14. The fibres are hollow and have pores along blood purification as it is continuously replaced.
their length with a size of 15,000–30,000 daltons. This Filter membrane polymers are of different materials:
allows plasma water to pass through, carrying dissolved AN69 (acrylonitrile/sodium methallyl sulfonate), PAN
wastes out of the blood (most of which have a molecular (polyacrylonitrile) or PA (polyamide), and polysulfone;
74
however, all demonstrate similar artificial kidney effects
and are generally applied according to the physician’s
42
Dialysate CVVHD(F)-diffusion and convection preference. The most important characteristics of filters
used in continuous modes of therapy are: (a) a high
Replacement plasma water clearance rate at low blood flow rates and
Fluids circuit pressures; and (b) high permeability to middle-
Heater sized molecular weight substances (500–15,000 daltons,
e.g. inflammatory cytokines), which are often encoun-
Blood tered in critical illness.
Pump
Vascular Access
As previously noted, in order to establish CRRT it is neces-
sary to create a blood flow outside the body using the EC.
Blood is most commonly accessed from the venous circu-
lation of the critical care patient via a catheter placed in a
Heater
Diafiltrate central vein (e.g. femoral). Blood is both withdrawn from
the vein and returned to the same vein – that is, veno-
venous (VV) access by means of a double (dual)-lumen
catheter. When the same procedure is carried out by
70
FIGURE 18.13 Continuous veno-venous haemodiafiltration (CVVHDf)
circuit. accessing the blood from the patient’s systemic circulation
Membrane casing Blood space
Potting agent Fibre holes
(blood flow)
Membrane fibre Blood tubing
connection
Port for dialysate or plasma
water removal
FIGURE 18.14 Haemofilter (dialysis membrane). Cross-sectional view indicating longitudinal synthetic fibres conveying blood into and out of the plastic
casing outer structure. Plasma water is removed via the side ultrafiltrate port during CVVH applying convective clearance. In CVVHDf, the blood is exposed
to fluid via the membrane fibres so that diffusive clearance can occur.