
Page 1331 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 1331
Chapter 72 Mast Cells and Mastocytosis 1177
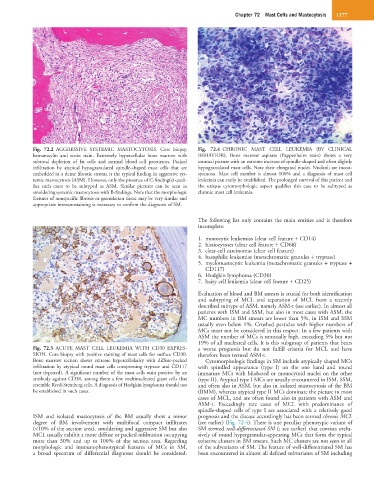
Fig. 72.2 AGGRESSIVE SYSTEMIC MASTOCYTOSIS. Core biopsy, Fig. 72.4 CHRONIC MAST CELL LEUKEMIA (BY CLINICAL
hematoxylin and eosin stain. Extremely hypercellular bone marrow with BEHAVIOR). Bone marrow aspirate (Pappenheim stain) shows a very
subtotal depletion of fat cells and normal blood cell precursors. Packed unusual picture with an extreme increase of spindle-shaped and often slightly
infiltration by atypical hypogranulated spindle-shaped mast cells that are hypogranulated mast cells. Note their elongated nuclei. Nucleoli are incon-
embedded in a dense fibrotic stroma is the typical finding in aggressive sys- spicuous. Mast cell number is almost 100% and a diagnosis of mast cell
temic mastocytosis (ASM). However, only the presence of C-finding(s) quali- leukemia can easily be established. The prolonged survival of this patient and
fies such cases to be subtyped as ASM. Similar pictures can be seen in the unique cytomorphologic aspect qualifies this case to be subtyped as
smoldering systemic mastocytosis with B-findings. Note that the morphologic chronic mast cell leukemia.
features of nonspecific fibrosis or granulation tissue may be very similar and
appropriate immunostaining is necessary to confirm the diagnosis of SM.
The following list only contains the main entities and is therefore
incomplete:
1. monocytic leukemias (clear cell feature + CD14)
2. histiocytoses (clear cell feature + CD68)
3. clear-cell carcinomas (clear cell feature)
4. basophilic leukemias (metachromatic granules + tryptase)
5. myelomastocytic leukemia (metachromatic granules + tryptase +
CD117)
6. Hodgkin lymphoma (CD30)
7. hairy cell leukemia (clear cell feature + CD25)
Evaluation of blood and BM smears is crucial for both identification
and subtyping of MCL and separation of MCL from a recently
described subtype of ASM, namely ASM-t (see earlier). In almost all
patients with ISM and SSM, but also in most cases with ASM, the
MC numbers in BM smears are lower than 5%, in ISM and SSM
usually even below 1%. Crushed particles with higher numbers of
MCs must not be considered in this respect. In a few patients with
ASM the number of MCs is unusually high, exceeding 5% but not
19% of all nucleated cells. It is this subgroup of patients that bears
Fig. 72.3 ACUTE MAST CELL LEUKEMIA WITH CD30 EXPRES- a worse prognosis but do not fulfill criteria for MCL and have
SION. Core biopsy with positive staining of mast cells for surface CD30. therefore been termed ASM-t.
Bone marrow section shows extreme hypercellularity with diffuse-packed Cytomorphologic findings in SM include atypically shaped MCs
infiltration by atypical round mast cells coexpressing tryptase and CD117 with spindled appearance (type I) on the one hand and round
(not depicted). A significant number of the mast cells stain positive by an immature MCs with bilobated or monocytoid nuclei on the other
antibody against CD30, among them a few multinucleated giant cells that (type II). Atypical type I MCs are usually encountered in ISM, SSM,
resemble Reed-Sternberg cells. A diagnosis of Hodgkin lymphoma should not and often also in ASM, but also in isolated mastocytosis of the BM
be established in such cases. (BMM), whereas atypical type II MCs dominate the picture in most
cases of MCL, and are often found also in patients with ASM and
ASM-t. Exceedingly rare cases of MCL with predominance of
spindle-shaped cells of type I are associated with a relatively good
ISM and isolated mastocytosis of the BM usually show a minor prognosis and the disease accordingly has been termed chronic MCL
degree of BM involvement with multifocal compact infiltrates (see earlier) (Fig. 72.4). There is one peculiar phenotypic variant of
(<10% of the section area), smoldering and aggressive SM but also SM termed well-differentiated SM (; see earlier) that consists exclu-
MCL usually exhibit a more diffuse or packed infiltration occupying sively of round hypergranular-appearing MCs that form the typical
more than 30% and up to 100% of the section area. Regarding cohesive clusters in BM smears. Such MC clusters are not seen in all
morphologic and immunophenotypical features of MCs in SM, of the subvariants of SM. The feature of well-differentiated SM has
a broad spectrum of differential diagnoses should be considered. been encountered in almost all defined subvariants of SM including