
Page 2131 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 2131
1892 Part XII Hemostasis and Thrombosis
Kallikrein
Factor XII
NH 2 Fibronectin II EGF1 Fibronectin I EGF2 K Catalytic domain COOH
S S
Prekallikrein R371 – I372
NH 2 Apple 1 Apple 2 Apple 3 Apple 4 Catalytic domain COOH
S S
Kininogen L362 – R363 R371 – S372
NH 2 D1 D2 D3 D4 D5 D6 COOH
“Bradykinin” “Surface-binding domain” “PK and FXI binding”
1 S S
HMW
1 Light chain 254
LMW and HMW
1 362 1 LMW 37
Heavy chain
Factor XI
R369 – I370
NH 2 Apple 1 Apple 2 Apple 3 Apple 4 Catalytic domain COOH
S S 2
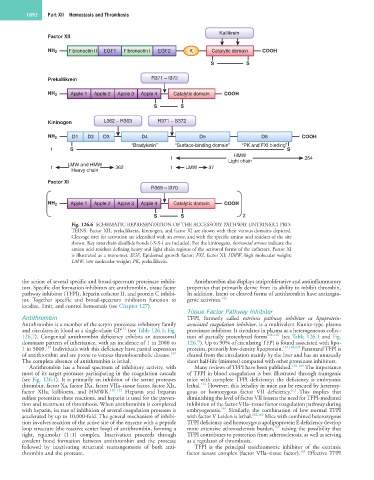
Fig. 126.6 SCHEMATIC REPRESENTATION OF THE ACCESSORY PATHWAY (INTRINSIC) PRO-
TEINS. Factor XII, prekallikrein, kininogen, and factor XI are shown with their various domains depicted.
Cleavage sites for activation are identified with an arrow, and with the specific amino acid residues of the site
shown. Key interchain disulfide bonds (-S-S-) are included. For the kininogens, horizontal arrows indicate the
amino acid residues defining heavy and light chain regions of the activated forms of the cofactors. Factor XI
is illustrated as a monomer. EGF, Epidermal growth factor; FXI, factor XI; HMW, high molecular weight;
LMW, low molecular weight; PK, prekallikrein.
the action of several specific and broad-spectrum proteinase inhibi- Antithrombin also displays antiproliferative and antiinflammatory
tors. Specific clot formation inhibitors are antithrombin, tissue factor properties that primarily derive from its ability to inhibit thrombin.
pathway inhibitor (TFPI), heparin cofactor II, and protein C inhibi- In addition, latent or cleaved forms of antithrombin have antiangio-
tor. Together specific and broad-spectrum inhibitors function to genic activities. 143
localize, limit, and control hemostasis (see Chapter 127).
Tissue Factor Pathway Inhibitor
Antithrombin TFPI, formerly called extrinsic pathway inhibitor or lipoprotein-
Antithrombin is a member of the serpin proteinase inhibitory family associated coagulation inhibitor, is a multivalent Kunitz-type plasma
137
and circulates in blood as a single-chain GP (see Table 126.1; Fig. proteinase inhibitor. It circulates in plasma as a heterogeneous collec-
126.7). Congenital antithrombin deficiency exhibits an autosomal tion of partially proteolyzed forms 144–147 (see Table 126.1 and Fig.
dominant pattern of inheritance, with an incidence of 1 in 2000 to 126.7). Up to 90% of circulating TFPI is found associated with lipo-
138
1 in 5000. Individuals with this deficiency have partial expression proteins, primarily low-density lipoprotein. 144,148,149 Parenteral TFPI is
139
of antithrombin and are prone to venous thromboembolic disease. cleared from the circulation mainly by the liver and has an unusually
The complete absence of antithrombin is lethal. short half-life (minutes) compared with other proteinase inhibitors.
Antithrombin has a broad spectrum of inhibitory activity, with Many reviews of TFPI have been published. 150–160 The importance
most of its target proteases participating in the coagulation cascade of TFPI in blood coagulation is best illustrated through transgenic
(see Fig. 126.1). It is primarily an inhibitor of the serine proteases mice with complete TFPI deficiency; the deficiency is embryonic
154
thrombin, factor Xa, factor IXa, factor VIIa–tissue factor, factor XIa, lethal. However, this lethality in mice can be rescued by heterozy-
161
factor XIIa, kallikrein, and HMWK. 140–142 Heparin and heparan gous or homozygous factor VII deficiency. This implies that
sulfate potentiate these reactions, and heparin is used for the preven- diminishing the level of factor VII lessens the need for TFPI-mediated
tion and treatment of thrombosis. When antithrombin is complexed inhibition of the factor VIIa–tissue factor coagulation pathway during
161
with heparin, its rate of inhibition of several coagulation proteases is embryogenesis. Similarly, the combination of low normal TFPI
accelerated by up to 10,000-fold. The general mechanism of inhibi- with factor V Leiden is lethal. 162,163 Mice with combined heterozygous
tion involves reaction of the active site of the enzyme with a peptide TFPI deficiency and homozygous apolipoprotein E deficiency develop
164
loop structure (the reactive center loop) of antithrombin, forming a more extensive atherosclerosis burden, raising the possibility that
tight, equimolar (1 : 1) complex. Inactivation proceeds through TFPI contributes to protection from atherosclerosis, as well as serving
covalent bond formation between antithrombin and the protease as a regulator of thrombosis.
followed by inactivating structural rearrangements of both anti- TFPI is the principal stoichiometric inhibitor of the extrinsic
165
thrombin and the protease. factor tenase complex (factor VIIa–tissue factor). Effective TFPI