
Page 1616 - Williams Hematology ( PDFDrive )
P. 1616
1590 Part XI: Malignant Lymphoid Diseases Chapter 96: Pathology of Lymphomas 1591
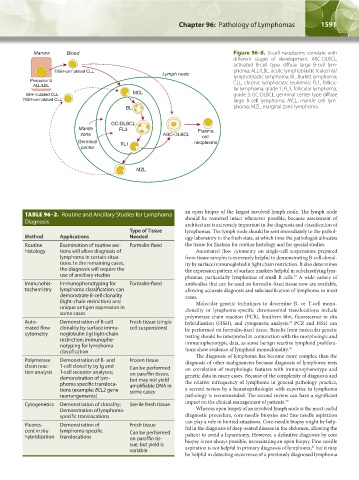
Marrow Blood Figure 96–8. B-cell neoplasms correlate with
different stages of development. ABC-DLBCL,
activated B-cell type diffuse large B-cell lym-
?IGH-unmutated CLL phoma; ALL/LBL, acute lymphoblastic leukemia/
Lymph node lymphoblastic lymphoma; BL, Burkitt lymphoma;
Precursor B CLL, chronic lymphocytic leukemia; FL1, follicu-
ALL/LBL lar lymphoma, grade 1; FL3, follicular lymphoma,
IGH-mutated CLL MCL grade 3; GC-DLBCL, germinal center type diffuse
?IGH-unmutated CLL large B-cell lymphoma; MCL, mantle cell lym-
BL phoma; MZL, marginal zone lymphoma.
GC-DLBCL
Mantle FL3 Plasma
zone ABC-DLBCL cell
Germinal FL1 neoplasms
center
MZL
TABLE 96–2. Routine and Ancillary Studies for Lymphoma an open biopsy of the largest involved lymph node. The lymph node
should be removed intact whenever possible, because assessment of
Diagnosis architecture is extremely important in the diagnosis and classification of
Type of Tissue lymphomas. The lymph node should be sent immediately to the pathol-
Method Applications Needed ogy laboratory in the fresh state, at which time the pathologist allocates
Routine Examination of routine sec- Formalin-fixed the tissue for fixation for routine histology and for special studies.
histology tions will allow diagnosis of Automated flow cytometry on single-cell suspensions prepared
lymphoma in certain situa- from tissue samples is extremely helpful in demonstrating B-cell clonal-
tions. In the remaining cases, ity by surface immunoglobulin light chain restriction. It also determines
the diagnosis will require the the expression pattern of surface markers helpful in subclassifying lym-
use of ancillary studies phomas, particularly lymphomas of small B cells. A wide variety of
17
Immunohis- Immunophenotyping for Formalin-fixed antibodies that can be used on formalin-fixed tissue now are available,
tochemistry lymphoma classification; can allowing accurate diagnosis and subclassification of lymphoma in most
demonstrate B-cell clonality cases.
(light-chain restriction) and Molecular genetic techniques to determine B- or T-cell mono-
unique antigen expression in clonality or lymphoma-specific chromosomal translocations include
some cases
polymerase chain reaction (PCR), Southern blot, fluorescence in situ
Auto- Demonstration of B-cell Fresh tissue (single hybridization (FISH), and cytogenetic analysis. PCR and FISH can
18
mated flow clonality by surface immu- cell suspensions) be performed on formalin-fixed tissue. Results from molecular genetic
cytometry noglobulin (Ig) light-chain testing should be interpreted in conjunction with the morphologic and
restriction; immunophe- immunophenotypic data, as some benign reactive lymphoid prolifera-
notyping for lymphoma 19
classification tions show evidence of lymphoid monoclonality.
The diagnosis of lymphoma has become more complex than the
Polymerase Demonstration of B- and Frozen tissue diagnosis of other malignancies because diagnosis of lymphoma rests
chain reac- T-cell clonality by Ig and Can be performed on correlation of morphologic features with immunophenotype and
tion analysis T-cell receptor analyses; on paraffin tissue,
demonstration of lym- but may not yield genetic data in many cases. Because of the complexity of diagnosis and
phoma specific transloca- amplifiable DNA in the relative infrequency of lymphoma in general pathology practice,
tions (example: BCL2 gene some cases a second review by a hematopathologist with expertise in lymphoma
rearrangements) pathology is recommended. The second review can have a significant
Cytogenetics Demonstration of clonality; Sterile fresh tissue impact on the clinical management of patients. 20
Demonstration of lymphoma- Whereas open biopsy of an involved lymph node is the most useful
specific translocations diagnostic procedure, core-needle biopsies and fine-needle aspiration
Fluores- Demonstration of Fresh tissue can play a role in limited situations. Core-needle biopsy might be help-
cent in situ lymphoma-specific Can be performed ful in the diagnosis of deep-seated disease in the abdomen, allowing the
hybridization translocations on paraffin tis- patient to avoid a laparotomy. However, a definitive diagnosis by core
sue, but yield is biopsy is not always possible, necessitating an open biopsy. Fine-needle
21
variable aspiration is not helpful in primary diagnosis of lymphoma, but it may
be helpful in detecting recurrence of a previously diagnosed lymphoma
Kaushansky_chapter 96_p1587-1602.indd 1591 9/18/15 6:07 PM