
Page 599 - Clinical Immunology_ Principles and Practice ( PDFDrive )
P. 599
CHaPTEr 41 Immunological Mechanisms of Airway Diseases and Pathways to Therapy 577
Antigen
IgE
FcεRI
B cell
IL-4
IL-13 Mast cell Upper airway
Histamine
Leukotrienes
Prostaglandins
cell Antigen
Th 2
Cytokines
FcεRI
IL-5
Allergic airway disease
Type 4 hypersensitivity
Eosinophil IL-4
IL-4Rα
Type 1 hypersensitivity IL-13
Lower airway
Th cell
2
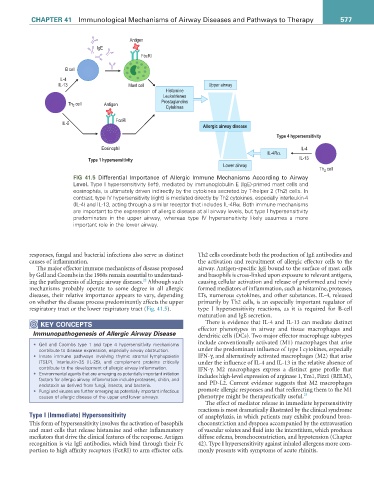
FIG 41.5 Differential Importance of Allergic Immune Mechanisms According to Airway
Level. Type I hypersensitivity (left), mediated by immunoglobulin E (IgE)-primed mast cells and
eosinophils, is ultimately driven indirectly by the cytokines secreted by T-helper 2 (Th2) cells. In
contrast, type IV hypersensitivity (right) is mediated directly by Th2 cytokines, especially interleukin-4
(IL-4) and IL-13, acting through a similar receptor that includes IL-4Rα. Both immune mechanisms
are important to the expression of allergic disease at all airway levels, but type I hypersensitivity
predominates in the upper airway, whereas type IV hypersensitivity likely assumes a more
important role in the lower airway.
responses, fungal and bacterial infections also serve as distinct Th2 cells coordinate both the production of IgE antibodies and
causes of inflammation. the activation and recruitment of allergic effector cells to the
The major effector immune mechanisms of disease proposed airway. Antigen-specific IgE bound to the surface of mast cells
by Gell and Coombs in the 1960s remain essential to understand- and basophils is cross-linked upon exposure to relevant antigens,
22
ing the pathogenesis of allergic airway diseases. Although such causing cellular activation and release of preformed and newly
mechanisms probably operate to some degree in all allergic formed mediators of inflammation, such as histamine, proteases,
diseases, their relative importance appears to vary, depending LTs, numerous cytokines, and other substances. IL-4, released
on whether the disease process predominantly affects the upper primarily by Th2 cells, is an especially important regulator of
respiratory tract or the lower respiratory tract (Fig. 41.5). type I hypersensitivity reactions, as it is required for B-cell
maturation and IgE secretion.
KEY CONCEPTS There is evidence that IL-4 and IL-13 can mediate distinct
Immunopathogenesis of Allergic Airway Disease effector phenotypes in airway and tissue macrophages and
dendritic cells (DCs). Two major effector macrophage subtypes
• Gell and Coombs type 1 and type 4 hypersensitivity mechanisms include conventionally activated (M1) macrophages that arise
contribute to disease expression, especially airway obstruction. under the predominant influence of type I cytokines, especially
• Innate immune pathways involving thymic stromal lymphopoietin IFN-γ, and alternatively activated macrophages (M2) that arise
(TSLP), interleukin-25 (IL-25), and complement proteins critically under the influence of IL-4 and IL-13 in the relative absence of
contribute to the development of allergic airway inflammation. IFN-γ. M2 macrophages express a distinct gene profile that
• Environmental agents that are emerging as potentially important initiation includes high-level expression of arginase 1, Ym1, Fizz1 (RELM),
factors for allergic airway inflammation include proteases, chitin, and
endotoxin as derived from fungi, insects, and bacteria. and PD-L2. Current evidence suggests that M2 macrophages
• Fungi and viruses are further emerging as potentially important infectious promote allergic responses and that redirecting them to the M1
causes of allergic disease of the upper and lower airways. phenotype might be therapeutically useful. 23
The effect of mediator release in immediate hypersensitivity
reactions is most dramatically illustrated by the clinical syndrome
Type I (Immediate) Hypersensitivity of anaphylaxis, in which patients may exhibit profound bron-
This form of hypersensitivity involves the activation of basophils choconstriction and dyspnea accompanied by the extravasation
and mast cells that release histamine and other inflammatory of vascular solutes and fluid into the interstitium, which produces
mediators that drive the clinical features of the response. Antigen diffuse edema, bronchoconstriction, and hypotension (Chapter
recognition is via IgE antibodies, which bind through their Fc 42). Type I hypersensitivity against inhaled allergens more com-
portion to high affinity receptors (FcεRI) to arm effector cells. monly presents with symptoms of acute rhinitis.