
Page 1830 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1830
CHAPTER 129: Dermatologic Conditions 1299
The purpura seen in meningococcemia result from two mechanisms.
The first is thrombosis precipitated by meningococcus, fibrin, and leu-
kocytes with a corresponding leukocytoclastic vasculitis. Thrombi are
concentrated in the lung, skin, spleen, heart, and liver. The second is
DIC precipitated by meningococcal endotoxin. Fibrin thrombi within
110
a vessel and a corresponding vasculitis are seen on histology.
Mortality rates are high and fewer than 30% with septic shock survive,
making an early diagnosis crucial. The Gram stain from a skin biopsy is
significantly more sensitive (72%) than the Gram stain from CSF (22%)
for detecting meningococci. Cultures should be sent from both blood and
skin biopsies. Mortality rates increase with extensive skin hemorrhage
(purpura fulminans, Fig. 129-24). Prompt antibiotic treatment is essen-
tial and improves outcomes. Third-generation cephalosporins should be
used empirically until culture results are available. Although antibiotic
therapy may decrease the yield of CSF cultures, it will not affect cultures
from the skin biopsies. Chloramphenicol is an acceptable alternative in
penicillin-allergic patients, although resistance has been reported. 111
■ INFECTIVE ENDOCARDITIS
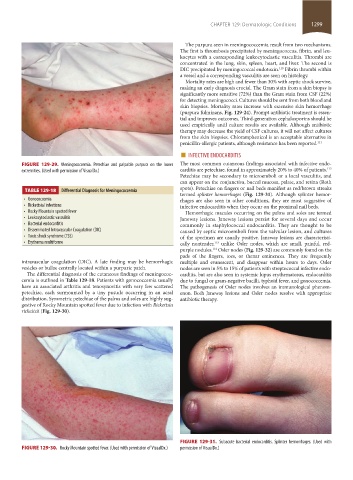
FIGURE 129-29. Meningococcemia. Petechiae and palpable purpura on the lower The most common cutaneous findings associated with infective endo-
112
extremities. (Used with permission of VisualDx.) carditis are petechiae, found in approximately 20% to 40% of patients.
Petechiae may be secondary to microemboli or a local vasculitis, and
can appear on the conjunctiva, buccal mucosa, palate, and retina (Roth
spots). Petechiae on fingers or nail beds manifest as red/brown streaks
TABLE 129-18 Differential Diagnosis for Meningococcemia
termed splinter hemorrhages (Fig. 129-31). Although splinter hemor-
• Gonococcemia rhages are also seen in other conditions, they are most suggestive of
• Rickettsial infections infective endocarditis when they occur on the proximal nail beds.
• Rocky Mountain spotted fever Hemorrhagic macules occurring on the palms and soles are termed
• Leukocytoclastic vasculitis Janeway lesions. Janeway lesions persist for several days and occur
• Bacterial endocarditis commonly in staphylococcal endocarditis. They are thought to be
• Disseminated Intravascular Coagulation (DIC) caused by septic microemboli from the valvular lesion, and cultures
• Toxic shock syndrome (TSS) of the specimen are usually positive. Janeway lesions are characteristi-
• Erythema multiforme cally nontender, unlike Osler nodes, which are small, painful, red-
113
purple nodules. Osler nodes (Fig. 129-32) are commonly found on the
114
pads of the fingers, toes, or thenar eminences. They are frequently
intravascular coagulation (DIC). A late finding may be hemorrhagic multiple and evanescent, and disappear within hours to days. Osler
vesicles or bullae centrally located within a purpuric patch. nodes are seen in 5% to 15% of patients with streptococcal infective endo-
The differential diagnosis of the cutaneous findings of meningococ- carditis, but are also seen in systemic lupus erythematosus, endocarditis
cemia is outlined in Table 129-18. Patients with gonococcemia usually due to fungal or gram-negative bacilli, typhoid fever, and gonococcemia.
have an associated arthritis and tenosynovitis with very few scattered The pathogenesis of Osler nodes involves an immunological phenom-
petechiae, each surmounted by a tiny pustule occurring in an acral enon. Both Janeway lesions and Osler nodes resolve with appropriate
distribution. Symmetric petechiae of the palms and soles are highly sug- antibiotic therapy.
gestive of Rocky Mountain spotted fever due to infection with Rickettsia
rickettsii (Fig. 129-30).
FIGURE 129-31. Subacute bacterial endocarditis. Splinter hemorrhages. (Used with
FIGURE 129-30. Rocky Mountain spotted fever. (Used with permission of VisualDx.) permission of VisualDx.)
section11.indd 1299 1/19/2015 10:55:32 AM