
Page 436 - Textbook of Pathology, 6th Edition
P. 436
420
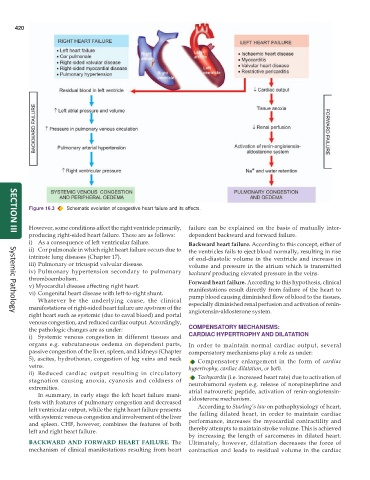
Figure 16.3 Schematic evolution of congestive heart failure and its effects.
However, some conditions affect the right ventricle primarily, failure can be explained on the basis of mutually inter-
producing right-sided heart failure. These are as follows: dependent backward and forward failure.
SECTION III
i) As a consequence of left ventricular failure. Backward heart failure. According to this concept, either of
ii) Cor pulmonale in which right heart failure occurs due to the ventricles fails to eject blood normally, resulting in rise
intrinsic lung diseases (Chapter 17). of end-diastolic volume in the ventricle and increase in
iii) Pulmonary or tricuspid valvular disease. volume and pressure in the atrium which is transmitted
iv) Pulmonary hypertension secondary to pulmonary backward producing elevated pressure in the veins.
thromboembolism. Forward heart failure. According to this hypothesis, clinical
v) Myocardial disease affecting right heart. manifestations result directly from failure of the heart to
vi) Congenital heart disease with left-to-right shunt. pump blood causing diminished flow of blood to the tissues,
Whatever be the underlying cause, the clinical
manifestations of right-sided heart failure are upstream of the especially diminished renal perfusion and activation of renin-
angiotensin-aldosterone system.
right heart such as systemic (due to caval blood) and portal
Systemic Pathology
venous congestion, and reduced cardiac output. Accordingly,
the pathologic changes are as under: COMPENSATORY MECHANISMS:
i) Systemic venous congestion in different tissues and CARDIAC HYPERTROPHY AND DILATATION
organs e.g. subcutaneous oedema on dependent parts, In order to maintain normal cardiac output, several
passive congestion of the liver, spleen, and kidneys (Chapter compensatory mechanisms play a role as under:
5), ascites, hydrothorax, congestion of leg veins and neck Compensatory enlargement in the form of cardiac
veins. hypertrophy, cardiac dilatation, or both.
ii) Reduced cardiac output resulting in circulatory Tachycardia (i.e. increased heart rate) due to activation of
stagnation causing anoxia, cyanosis and coldness of neurohumoral system e.g. release of norepinephrine and
extremities. atrial natrouretic peptide, activation of renin-angiotensin-
In summary, in early stage the left heart failure mani-
fests with features of pulmonary congestion and decreased aldosterone mechanism.
left ventricular output, while the right heart failure presents According to Starling’s law on pathophysiology of heart,
with systemic venous congestion and involvement of the liver the failing dilated heart, in order to maintain cardiac
and spleen. CHF, however, combines the features of both performance, increases the myocardial contractility and
left and right heart failure. thereby attempts to maintain stroke volume. This is achieved
by increasing the length of sarcomeres in dilated heart.
BACKWARD AND FORWARD HEART FAILURE. The Ultimately, however, dilatation decreases the force of
mechanism of clinical manifestations resulting from heart contraction and leads to residual volume in the cardiac