
Page 679 - Textbook of Pathology, 6th Edition
P. 679
663
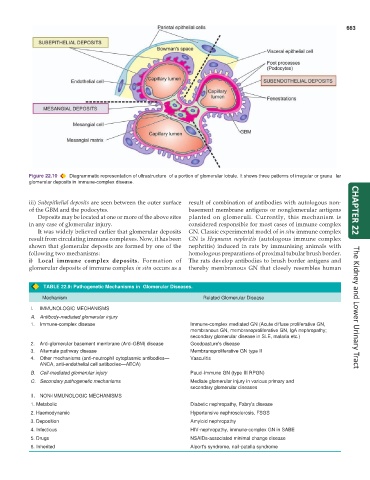
Figure 22.10 Diagrammatic representation of ultrastructure of a portion of glomerular lobule. It shows three patterns of irregular or granu lar
glomerular deposits in immune-complex disease.
iii) Subepithelial deposits are seen between the outer surface result of combination of antibodies with autologous non-
of the GBM and the podocytes. basement membrane antigens or nonglomerular antigens CHAPTER 22
Deposits may be located at one or more of the above sites planted on glomeruli. Currently, this mechanism is
in any case of glomerular injury. considered responsible for most cases of immune complex
It was widely believed earlier that glomerular deposits GN. Classic experimental model of in situ immune complex
result from circulating immune complexes. Now, it has been GN is Heymann nephritis (autologous immune complex
shown that glomerular deposits are formed by one of the nephritis) induced in rats by immunising animals with
following two mechanisms: homologous preparations of proximal tubular brush border.
i) Local immune complex deposits. Formation of The rats develop antibodies to brush border antigens and
glomerular deposits of immune complex in situ occurs as a thereby membranous GN that closely resembles human
TABLE 22.9: Pathogenetic Mechanisms in Glomerular Diseases.
Mechanism Related Glomerular Disease
I. IMMUNOLOGIC MECHANISMS The Kidney and Lower Urinary Tract
A. Antibody-mediated glomerular injury
1. Immune-complex disease Immune-complex mediated GN (Acute diffuse proliferative GN,
membranous GN, membranoproliferative GN, IgA nephropathy;
secondary glomerular disease in SLE, malaria etc.)
2. Anti-glomerular basement membrane (Anti-GBM) disease Goodpasture's disease
3. Alternate pathway disease Membranoproliferative GN type II
4. Other mechanisms (anti-neutrophil cytoplasmic antibodies— Vasculitis
ANCA, anti-endothelial cell antibodies—AECA)
B. Cell-mediated glomerular injury Pauci-immune GN (type III RPGN)
C. Secondary pathogenetic mechanisms Mediate glomerular injury in various primary and
secondary glomerular diseases
II. NON-IMMUNOLOGIC MECHANISMS
1. Metabolic Diabetic nephropathy, Fabry's disease
2. Haemodynamic Hypertensive nephrosclerosis, FSGS
3. Deposition Amyloid nephropathy
4. Infectious HIV-nephropathy, immune-complex GN in SABE
5. Drugs NSAIDs-associated minimal change disease
6. Inherited Alport's syndrome, nail-patella syndrome