
Page 712 - Textbook of Pathology, 6th Edition
P. 712
696
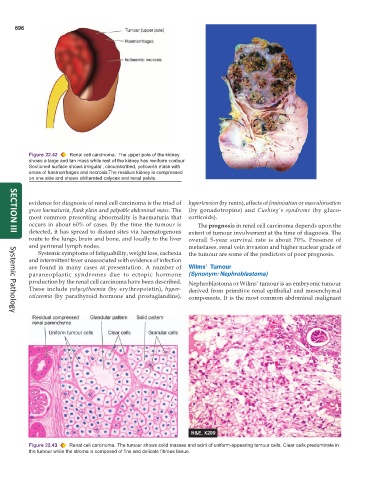
Figure 22.42 Renal cell carcinoma. The upper pole of the kidney
shows a large and tan mass while rest of the kidney has reniform contour
.
Sectioned surface shows irregular , circumscribed, yellowish mass with
areas of haemorrhages and necrosis. The residual kidney is compressed
on one side and shows obliterated calyces and renal pelvis.
evidence for diagnosis of renal cell carcinoma is the triad of hypertension (by renin), effects of feminisation or masculinisation
gross haematuria, flank plain and palpable abdominal mass. The (by gonadotropins) and Cushing’s syndrome (by gluco-
most common presenting abnormality is haematuria that corticoids).
occurs in about 60% of cases. By the time the tumour is The prognosis in renal cell carcinoma depends upon the
detected, it has spread to distant sites via haematogenous extent of tumour involvement at the time of diagnosis. The
SECTION III
route to the lungs, brain and bone, and locally to the liver overall 5-year survival rate is about 70%. Presence of
and perirenal lymph nodes. metastases, renal vein invasion and higher nuclear grade of
Systemic symptoms of fatiguability, weight loss, cachexia the tumour are some of the predictors of poor prognosis.
and intermittent fever unassociated with evidence of infection
are found in many cases at presentation. A number of Wilms’ Tumour
paraneoplastic syndromes due to ectopic hormone (Synonym: Nephroblastoma)
production by the renal cell carcinoma have been described. Nephroblastoma or Wilms’ tumour is an embryonic tumour
These include polycythaemia (by erythropoietin), hyper- derived from primitive renal epithelial and mesenchymal
calcaemia (by parathyroid hormone and prostaglandins), components. It is the most common abdominal malignant
Systemic Pathology
Figure 22.43 Renal cell carcinoma. The tumour shows solid masses and acini of uniform-appearing tumour cells. Clear cells predominate in
the tumour while the stroma is composed of fine and delicate fibrous tissue.