
Page 840 - Textbook of Pathology, 6th Edition
P. 840
824 Type 1 DM: Pathogenesis of Complications
i) Patients of type 1 DM usually manifest at early age, It is now known that in both type 1 and 2 DM, severity and
generally below the age of 35. chronicity of hyperglycaemia forms the main pathogenetic
ii) The onset of symptoms is often abrupt. mechanism for ‘microvascular complications’ (e.g.
iii) At presentation, these patients have polyuria, polydipsia retinopathy, nephropathy, neuropathy); therefore control of
and polyphagia. blood glucose level constitutes the mainstay of treatment for
iv) The patients are not obese but have generally progressive minimising development of these complications.
loss of weight. Longstanding cases of type 2 DM, however, in addition,
v) These patients are prone to develop metabolic frequently develop ‘macrovascular complications’
complications such as ketoacidosis and hypoglycaemic (e.g. atherosclerosis, coronary artery disease, peripheral
episodes. vascular disease, cerebrovascular disease) which are more
difficult to explain on the basis of hyperglycaemia alone.
Type 2 DM: The following biochemical mechanisms have been
i) This form of diabetes generally manifests in middle life proposed to explain the development of complications of
or beyond, usually above the age of 40. diabetes mellitus (Fig. 27.26, A):
ii) The onset of symptoms in type 2 DM is slow and 1. Non-enzymatic protein glycosylation: The free amino
insidious. group of various body proteins binds by non-enzymatic
iii) Generally, the patient is asymptomatic when the mechanism to glucose; this process is called glycosylation and
diagnosis is made on the basis of glucosuria or hyper- is directly proportionate to the severity of hyperglycaemia.
glycaemia during physical examination, or may present with Various body proteins undergoing chemical alterations in
polyuria and polydipsia. this way include haemoglobin, lens crystalline protein, and
iv) The patients are frequently obese and have unexplained basement membrane of body cells. An example is the
weakness and loss of weight. measurement of a fraction of haemoglobin called
v) Metabolic complications such as ketoacidosis are glycosylated haemoglobin (HbA ) as a test for monitoring
1C
infrequent. glycaemic control in a diabetic patient during the preceding
SECTION III
Systemic Pathology
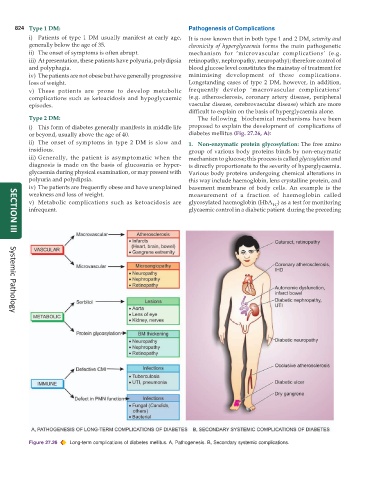
Figure 27.26 Long-term complications of diabetes mellitus. A, Pathogenesis. B, Secondary systemic complications.