
Page 836 - Textbook of Pathology, 6th Edition
P. 836
820
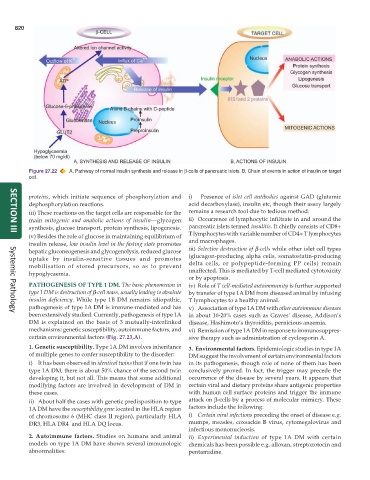
Figure 27.22 A, Pathway of normal insulin synthesis and release in β-cells of pancreatic islets. B, Chain of events in action of insulin on target
cell.
proteins, which initiate sequence of phosphorylation and i) Presence of islet cell antibodies against GAD (glutamic
dephosphorylation reactions. acid decarboxylase), insulin etc, though their assay largely
iii) These reactions on the target cells are responsible for the remains a research tool due to tedious method.
main mitogenic and anabolic actions of insulin—glycogen ii) Occurrence of lymphocytic infiltrate in and around the
synthesis, glucose transport, protein synthesis, lipogenesis. pancreatic islets termed insulitis. It chiefly consists of CD8+
iv) Besides the role of glucose in maintaining equilibrium of T lymphocytes with variable number of CD4+ T lymphocytes
SECTION III
insulin release, low insulin level in the fasting state promotes and macrophages.
hepatic gluconeogenesis and glycogenolysis, reduced glucose iii) Selective destruction of β-cells while other islet cell types
uptake by insulin-sensitive tissues and promotes (glucagon-producing alpha cells, somatostatin-producing
mobilisation of stored precursors, so as to prevent delta cells, or polypeptide-forming PP cells) remain
hypoglycaemia. unaffected. This is mediated by T-cell mediated cytotoxicity
or by apoptosis.
PATHOGENESIS OF TYPE 1 DM. The basic phenomenon in iv) Role of T cell-mediated autoimmunity is further supported
type 1 DM is destruction of β-cell mass, usually leading to absolute by transfer of type 1A DM from diseased animal by infusing
insulin deficiency. While type 1B DM remains idiopathic, T lymphocytes to a healthy animal.
pathogenesis of type 1A DM is immune-mediated and has v) Association of type 1A DM with other autoimmune diseases
been extensively studied. Currently, pathogenesis of type 1A in about 10-20% cases such as Graves’ disease, Addison’s
Systemic Pathology
DM is explained on the basis of 3 mutually-interlinked disease, Hashimoto’s thyroiditis, pernicious anaemia.
mechanisms: genetic susceptibility, autoimmune factors, and vi) Remission of type 1A DM in response to immunosuppres-
certain environmental factors (Fig. 27.23,A). sive therapy such as administration of cyclosporin A.
1. Genetic susceptibility. Type 1A DM involves inheritance 3. Environmental factors. Epidemiologic studies in type 1A
of multiple genes to confer susceptibility to the disorder: DM suggest the involvement of certain environmental factors
i) It has been observed in identical twins that if one twin has in its pathogenesis, though role of none of them has been
type 1A DM, there is about 50% chance of the second twin conclusively proved. In fact, the trigger may precede the
developing it, but not all. This means that some additional occurrence of the disease by several years. It appears that
modifying factors are involved in development of DM in certain viral and dietary proteins share antigenic properties
these cases. with human cell surface proteins and trigger the immune
ii) About half the cases with genetic predisposition to type attack on β-cells by a process of molecular mimicry. These
1A DM have the susceptibility gene located in the HLA region factors include the following:
of chromosome 6 (MHC class II region), particularly HLA i) Certain viral infections preceding the onset of disease e.g.
DR3, HLA DR4 and HLA DQ locus. mumps, measles, coxsackie B virus, cytomegalovirus and
infectious mononucleosis.
2. Autoimmune factors. Studies on humans and animal ii) Experimental induction of type 1A DM with certain
models on type 1A DM have shown several immunologic chemicals has been possible e.g. alloxan, streptozotocin and
abnormalities: pentamidine.