
Page 126 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 126
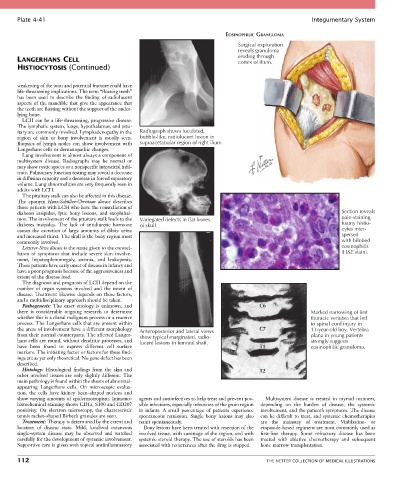
Plate 4-41 Integumentary System
EOSINOPHILIC GRANULOMA
Surgical exploration
reveals granuloma
LANGERHANS CELL eroding through
cortex of ilium.
HISTIOCYTOSIS (Continued)
weakening of the joint and potential fracture could have
life-threatening implications. The term “floating teeth”
has been used to describe the finding of radiolucent
aspects of the mandible that give the appearance that
the teeth are floating without the support of the under-
lying bone.
LCH can be a life-threatening, progressive disease.
The lymphatic system, lungs, hypothalamus, and pitu-
itary are commonly involved. Lymphadenopathy in the Radiograph shows loculated,
region of skin or bony involvement is usually seen. bubble-like, radiolucent lesion in
Biopsies of lymph nodes can show involvement with supraacetabular region of right ilium.
Langerhans cells or dermatopathic changes.
Lung involvement is almost always a component of
multisystem disease. Radiographs may be normal or
may show cystic spaces or a nonspecific interstitial infil-
trate. Pulmonary function testing may reveal a decrease
in diffusion capacity and a decrease in forced expiratory
volume. Lung abnormalities are very frequently seen in
adults with LCH.
The pituitary stalk can also be affected in this disease.
The eponym Hans-Schüller-Christian disease describes
those patients with LCH who have the constellation of
diabetes insipidus, lytic bony lesions, and exophthal- Section reveals
mos. The involvement of the pituitary stalk leads to the Variegated defects in flat bones pale-staining,
diabetes insipidus. The lack of antidiuretic hormone of skull foamy histio-
causes the excretion of large amounts of dilute urine cytes inter-
and increased thirst. The skull is the bony region most spersed
commonly involved. with bilobed
Letterer-Siwe disease is the name given to the constel- eosinophilis
lation of symptoms that include severe skin involve- (H&E stain).
ment, hepatosplenomegaly, anemia, and leukopenia.
These patients have early onset of disease in infancy and
have a poor prognosis because of the aggressiveness and
extent of the disease load.
The diagnosis and prognosis of LCH depend on the
number of organ systems involved and the extent of
disease. Treatment likewise depends on these factors,
and a multidisciplinary approach should be taken.
Pathogenesis: The exact etiology is unknown, and C6
there is considerable ongoing research to determine Marked narrowing of first
whether this is a clonal malignant process or a reactive thoracic vertebra that led
process. The Langerhans cells that are present within to spinal cord injury in
the areas of involvement have a different morphology Anteroposterior and lateral views C7 13-year-old boy. Vertebra
from their normal counterparts. The affected Langer- show typical marginated, radio- plana in young patients
hans cells are round, without dendritic processes, and lucent lesions in femoral shaft. strongly suggests
have been found to express different cell surface T1 eosinophilic granuloma.
markers. The initiating factor or factors for these find-
ings are as yet only theoretical. No gene defect has been
described.
Histology: Histological findings from the skin and T2
other involved tissues are only slightly different. The
main pathology is found within the sheets of abnormal-
appearing Langerhans cells. On microscopic evalua-
tion, the cells have kidney bean–shaped nucleus and
show varying amounts of epidermotropism. Immuno- agents and antiinfectives to help treat and prevent pos- Multisystem disease is treated in myriad manners,
histochemical staining shows CD1a, S100 and CD207 sible infections, especially infections of the groin region depending on the burden of disease, the systemic
positivity. On electron microscopy, the characteristic in infants. A small percentage of patients experience involvement, and the patient’s symptoms. The disease
tennis racket–shaped Birbeck granules are seen. spontaneous remission. Single bony lesions may also can be difficult to treat, and systemic chemotherapies
Treatment: Therapy is determined by the extent and remit spontaneously. are the mainstay of treatment. Vinblastine- or
location of disease state. Mild, localized cutaneous Bony lesions have been treated with resection of the etoposide-based regimens are most commonly used as
single-system disease may be observed and watched involved tissue, with curettage of the region, and with first-line therapy. Some refractory disease has been
carefully for the development of systemic involvement. systemic steroid therapy. The use of steroids has been treated with ablative chemotherapy and subsequent
Supportive care is given with topical antiinflammatory associated with recurrences after the drug is stopped. bone marrow transplantation.
112 THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS