
Page 193 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 193
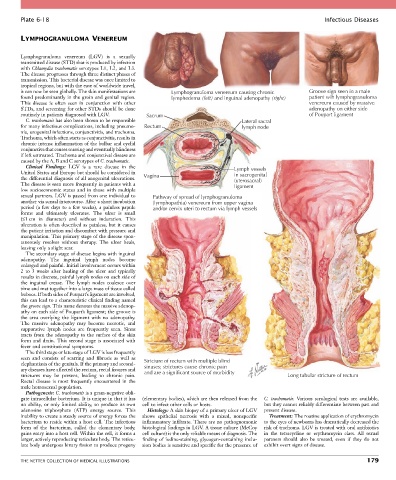
Plate 6-18 Infectious Diseases
LYMPHOGRANULOMA VENEREUM
Lymphogranuloma venereum (LGV) is a sexually
transmitted disease (STD) that is produced by infection
with Chlamydia trachomatis serotypes L1, L2, and L3.
The disease progresses through three distinct phases of
transmission. This bacterial disease was once limited to
tropical regions, but with the ease of worldwide travel,
it can now be seen globally. The skin manifestations are Lymphogranuloma venereum causing chronic Groove sign seen in a male
found predominantly in the groin and genital region. lymphedema (left) and inguinal adenopathy (right) patient wih lymphogranuloma
This disease is often seen in conjunction with other venereum caused by massive
STDs, and screening for other STDs should be done adenopathy on either side
routinely in patients diagnosed with LGV. Sacrum of Poupart ligament
C. trachomatis has also been shown to be responsible Lateral sacral
for many infectious complications, including pneumo- Rectum lymph node
nia, urogenital infections, conjunctivitis, and trachoma.
Trachoma, which often starts as conjunctivitis, results in
chronic intense inflammation of the bulbar and eyelid
conjunctiva that causes scarring and eventually blindness
if left untreated. Trachoma and conjunctival disease are
caused by the A, B and C serotypes of C. trachomatis.
Clinical Findings: LGV is a rare disease in the Lymph vessels
United States and Europe but should be considered in in sacrogenital
the differential diagnosis of all anogenital ulcerations. Vagina (uterosacral)
The disease is seen more frequently in patients with a ligament
low socioeconomic status and in those with multiple
sexual partners. LGV is passed from one individual to Pathway of spread of lymphogranuloma
another via sexual intercourse. After a short incubation (lymphopathia) venereum from upper vagina
period (a few days to a few weeks), a painless papule and/or cervix uteri to rectum via lymph vessels
forms and ultimately ulcerates. The ulcer is small
(≤1 cm in diameter) and without induration. This
ulceration is often described as painless, but it causes
the patient irritation and discomfort with pressure and
manipulation. This primary stage of the disease spon-
taneously resolves without therapy. The ulcer heals,
leaving only a slight scar.
The secondary stage of disease begins with inguinal
adenopathy. The inguinal lymph nodes become
enlarged and painful. Initial involvement occurs within
2 to 3 weeks after healing of the ulcer and typically
results in discrete, painful lymph nodes on each side of
the inguinal crease. The lymph nodes coalesce over
time and mat together into a large mass of tissue called
buboes. If both sides of Poupart’s ligament are involved,
this can lead to a characteristic clinical finding named
the groove sign. This name denotes the massive adenop-
athy on each side of Poupart’s ligament; the groove is
the area overlying the ligament with no adenopathy.
The massive adenopathy may become necrotic, and
suppurative lymph nodes are frequently seen. Sinus
tracts from the adenopathy to the surface of the skin
form and drain. This second stage is associated with
fever and constitutional symptoms.
The third stage or late stage of LGV is less frequently
seen and consists of scarring and fibrosis as well as Stricture of rectum with multiple blind
elephantiasis of the genitals. If the primary and second- sinuses; strictures cause chronic pain
ary diseases have affected the rectum, rectal fissures and and are a significant source of morbidity
strictures may be present, leading to chronic pain. Long tubular stricture of rectum
Rectal disease is most frequently encountered in the
male homosexual population.
Pathogenesis: C. trachomatis is a gram-negative obli-
gate intracellular bacterium. It is unique in that it has (elementary bodies), which are then released from the C. trachomatis. Various serological tests are available,
no ability, or only limited ability, to produce its own cell to infect other cells or hosts. but they cannot reliably differentiate between past and
adenosine triphosphate (ATP) energy source. This Histology: A skin biopsy of a primary ulcer of LGV present disease.
inability to create a steady source of energy forces the shows epithelial necrosis with a mixed, nonspecific Treatment: The routine application of erythromycin
bacterium to reside within a host cell. The infectious inflammatory infiltrate. There are no pathognomonic to the eyes of newborns has dramatically decreased the
form of the bacterium, called the elementary body, histological findings in LGV. A tissue culture (McCoy risk of trachoma. LGV is treated with oral antibiotics
gains entry into a host cell. Within the cell, it forms a cell culture) is the only reliable means of diagnosis. The in the tetracycline or erythromycin class. All sexual
larger, actively reproducing reticulate body. The reticu- finding of iodine-staining, glycogen-containing inclu- partners should also be treated, even if they do not
late body undergoes binary fission to produce progeny sion bodies is sensitive and specific for the presence of exhibit overt signs of disease.
THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS 179