
Page 200 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 200
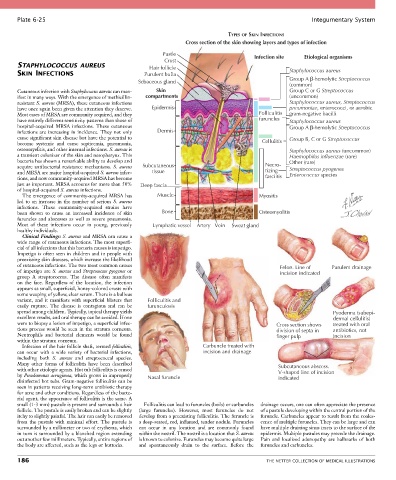
Plate 6-25 Integumentary System
TYPES OF SKIN INFECTIONS
Cross section of the skin showing layers and types of infection
Pustle Infection site Etiological organisms
Crust
STAPHYLOCOCCUS AUREUS Hair follicle
SKIN INFECTIONS Purulent bulla Staphylococcus aureus
Sebaceous gland Group A β-hemolytic Streptococcus
(common)
Cutaneous infection with Staphylococcus aureus can man- Skin Group C or G Streptococcus
ifest in many ways. With the emergence of methicillin- compartments (uncommon)
resistant S. aureus (MRSA), these cutaneous infections Staphylococcus aureus, Streptococcus
have once again been given the attention they deserve. Epidermis pneumoniae, enterococci, or aerobic
Most cases of MRSA are community acquired, and they Folliculitis gram-negative bacilli
have entirely different sensitivity patterns than those of furuncles Staphylococcus aureus
hospital-acquired MRSA infections. These cutaneous Group A β-hemolytic Streptococcus
infections are increasing in incidence. They not only Dermis
cause significant skin disease but have the potential to Group B, C or G Streptococcus
become systemic and cause septicemia, pneumonia, Cellulitis
osteomyelitis, and other internal infections. S. aureus is Staphylococcus aureus (uncommon)
a transient colonizer of the skin and nasopharynx. This Haemophilus influenzae (rare)
bacteria has shown a remarkable ability to develop and Other (rare)
acquire antibacterial resistance mechanisms. S. aureus Subcutaneous Necro- Streptococcus pyogenes
and MRSA are major hospital-acquired S. aureus infec- tissue tizing Enterococcus species
tions, and now community-acquired MRSA has become fasciitis
just as important. MRSA accounts for more than 50% Deep fascia
of hospital-acquired S. aureus infections.
The emergence of community-acquired MRSA has Muscle Myositis
led to an increase in the number of serious S. aureus
infections. These community-acquired strains have
been shown to cause an increased incidence of skin Bone Osteomyolitis
furuncles and abscesses as well as severe pneumonia.
Most of these infections occur in young, previously Lymphatic vessel Artery Vein Sweat gland
healthy individuals.
Clinical Findings: S. aureus and MRSA can cause a
wide range of cutaneous infections. The most superfi-
cial of all infections that this bacteria causes is impetigo.
Impetigo is often seen in children and in people with
preexisting skin diseases, which increase the likelihood
of cutaneous infections. The two most common causes Felon. Line of Purulent drainage
of impetigo are S. aureus and Streptococcus pyogenes or incision indicated
group A streptococcus. The disease often manifests
on the face. Regardless of the location, the infection
appears as small, superficial, honey-colored crusts with
some weeping of yellow, clear serum. There is a bullous
variant, and it manifests with superficial blisters that Folliculitis and
easily rupture. The disease is contagious and can be furunculosis
spread among children. Typically, topical therapy yields Pyoderma (subepi-
excellent results, and oral therapy can be avoided. If one dermal cellulitis)
were to biopsy a lesion of impetigo, a superficial infec- Cross section shows treated with oral
tious process would be seen in the stratum corneum. division of septa in antibiotics, not
Neutrophils and bacterial elements would be found finger pulp incision
within the stratum corneum.
Infection of the hair follicle shaft, termed folliculitis, Carbuncle treated with
can occur with a wide variety of bacterial infections, incision and drainage
including both S. aureus and streptococcal species.
Many other forms of folliculitis have been described Subcutaneous abscess.
with other etiologic agents. Hot tub folliculitis is caused V-shaped line of incision
by Pseudomonas aeruginosa, which grows in improperly Nasal furuncle indicated
disinfected hot tubs. Gram-negative folliculitis can be
seen in patients receiving long-term antibiotic therapy
for acne and other conditions. Regardless of the bacte-
rial agent, the appearance of folliculitis is the same. A
small (1-3 mm) pustule is present and surrounds a hair Folliculitis can lead to furuncles (boils) or carbuncles drainage occurs, one can often appreciate the presence
follicle. The pustule is easily broken and can be slightly (large furuncles). However, most furuncles do not of a pustule developing within the central portion of the
itchy to slightly painful. The hair can easily be removed develop from a preexisting folliculitis. The furuncle is furuncle. Carbuncles appear to result from the coales-
from the pustule with minimal effort. The pustule is a deep-seated, red, inflamed, tender nodule. Furuncles cence of multiple furuncles. They can be large and can
surrounded by a millimeter or two of erythema, which can occur in any location and are commonly found have multiple draining sinus tracts to the surface of the
in turn is surrounded by a blanched region extending within the nostril. The nostril is a location that S. aureus epidermis. Multiple pustules may precede the drainage.
out another few millimeters. Typically, entire regions of is known to colonize. Furuncles may become quite large Pain and localized adenopathy are hallmarks of both
the body are affected, such as the legs or buttocks. and spontaneously drain to the surface. Before the furuncles and carbuncles.
186 THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS