
Page 70 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 70
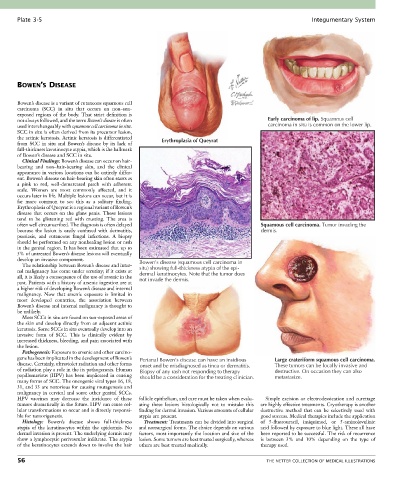
Plate 3-5 Integumentary System
BOWEN’S DISEASE
Bowen’s disease is a variant of cutaneous squamous cell
carcinoma (SCC) in situ that occurs on non–sun-
exposed regions of the body. That strict definition is
not always followed, and the term Bowen’s disease is often Early carcinoma of lip. Squamous cell
used interchangeably with squamous cell carcinoma in situ. carcinoma in situ is common on the lower lip.
SCC in situ is often derived from its precursor lesion,
the actinic keratosis. Actinic keratosis is differentiated Erythroplasia of Queyrat
from SCC in situ and Bowen’s disease by its lack of
full-thickness keratinocyte atypia, which is the hallmark
of Bowen’s disease and SCC in situ.
Clinical Findings: Bowen’s disease can occur on hair-
bearing and non–hair-bearing skin, and the clinical
appearance in various locations can be entirely differ-
ent. Bowen’s disease on hair-bearing skin often starts as
a pink to red, well-demarcated patch with adherent
scale. Women are most commonly affected, and it
occurs later in life. Multiple lesions can occur, but it is
far more common to see this as a solitary finding.
Erythroplasia of Queyrat is a regional variant of Bowen’s
disease that occurs on the glans penis. These lesions
tend to be glistening red with crusting. The area is
often well circumscribed. The diagnosis is often delayed Squamous cell carcinoma. Tumor invading the
because the lesion is easily confused with dermatitis, dermis.
psoriasis, and cutaneous fungal infections. A biopsy
should be performed on any nonhealing lesion or rash
in the genital region. It has been estimated that up to
5% of untreated Bowen’s disease lesions will eventually
develop an invasive component. Bowen’s disease (squamous cell carcinoma in
The relationship between Bowen’s disease and inter-
nal malignancy has come under scrutiny; if it exists at situ) showing full-thickness atypia of the epi-
dermal keratinocytes. Note that the tumor does
all, it is likely a consequence of the use of arsenic in the not invade the dermis.
past. Patients with a history of arsenic ingestion are at
a higher risk of developing Bowen’s disease and internal
malignancy. Now that arsenic exposure is limited in
most developed countries, the association between
Bowen’s disease and internal malignancy is thought to
be unlikely.
Most SCCs in situ are found on sun-exposed areas of
the skin and develop directly from an adjacent actinic
keratosis. Some SCCs in situ eventually develop into an
invasive form of SCC. This is clinically evident by
increased thickness, bleeding, and pain associated with
the lesion.
Pathogenesis: Exposure to arsenic and other carcino-
gens has been implicated in the development of Bowen’s Perianal Bowen’s disease can have an insidious Large crateriform squamous cell carcinoma.
disease. Certainly, ultraviolet radiation and other forms onset and be misdiagnosed as tinea or dermatitis. These tumors can be locally invasive and
of radiation play a role in the its pathogenesis. Human Biopsy of any rash not responding to therapy destructive. On occasion they can also
papillomavirus (HPV) has been implicated in causing should be a consideration for the treating clinician. metastasize.
many forms of SCC. The oncogenic viral types 16, 18,
31, and 33 are notorious for causing mutagenesis and
malignancy in cervical and some other genital SCCs.
HPV vaccines may decrease the incidence of these follicle epithelium, and care must be taken when evalu- Simple excision or electrodessication and curettage
tumors dramatically in the future. HPV can cause cel- ating these lesions histologically not to mistake this are highly effective treatments. Cryotherapy is another
lular transformations to occur and is directly responsi- finding for dermal invasion. Various amounts of cellular destructive method that can be selectively used with
ble for tumorigenesis. atypia are present. good success. Medical therapies include the application
Histology: Bowen’s disease shows full-thickness Treatment: Treatments can be divided into surgical of 5-fluorouracil, imiquimod, or 5-aminolevulinic
atypia of the keratinocytes within the epidermis. No and nonsurgical forms. The choice depends on various acid followed by exposure to blue light. These all have
dermal invasion is present. The underlying dermis may factors, most importantly the location and size of the been reported to be successful. The risk of recurrence
show a lymphocytic perivascular infiltrate. The atypia lesion. Some tumors are best treated surgically, whereas is between 3% and 10% depending on the type of
of the keratinocytes extends down to involve the hair others are best treated medically. therapy used.
56 THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS