
Page 71 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 71
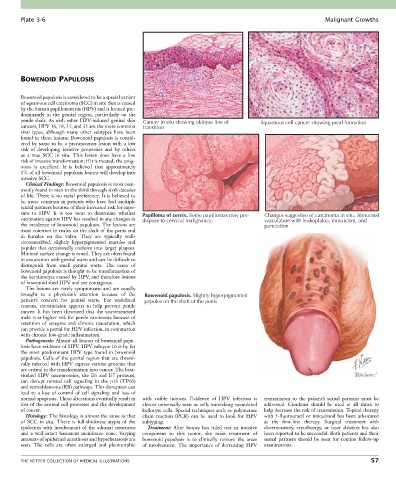
Plate 3-6 Malignant Growths
BOWENOID PAPULOSIS
Bowenoid papulosis is considered to be a special variant
of squamous cell carcinoma (SCC) in situ that is caused
by the human papillomavirus (HPV) and is located pre-
dominantly in the genital region, particularly on the
penile shaft. As with other HPV-induced genital skin Cancer in situ showing oblique line of Squamous cell cancer showing pearl formation
cancers, HPV 16, 18, 31, and 33 are the more common transition
viral types, although many other subtypes have been
found in these lesions. Bowenoid papulosis is consid-
ered by some to be a precancerous lesion with a low
risk of developing invasive properties and by others
as a true SCC in situ. This lesion does have a low
risk of invasive transformation; if it is treated, the prog-
nosis is excellent. It is believed that approximately
1% of all bowenoid papulosis lesions will develop into
invasive SCC.
Clinical Findings: Bowenoid papulosis is most com-
monly found in men in the third through sixth decades
of life. There is no racial preference. It is believed to
be more common in patients who have had multiple
sexual partners because of their increased risk for expo-
sure to HPV. It is too soon to determine whether Papilloma of cervix. Some papillomas may pre- Changes suggestive of carcinoma in situ. Abnormal
vaccination against HPV has resulted in any changes in dispose to cervical malignancy. vasculature with leukoplakia, mosaicism, and
the incidence of bowenoid papulosis. The lesions are punctation
most common in males on the shaft of the penis and
in females on the vulva. They are typically well-
circumscribed, slightly hyperpigmented macules and
papules that occasionally coalesce into larger plaques.
Minimal surface change is noted. They are often found
in association with genital warts and can be difficult to
distinguish from small genital warts. The cause of
bowenoid papulosis is thought to be transformation of
the keratinocyte caused by HPV, and therefore lesions
of bowenoid shed HPV and are contagious.
The lesions are rarely symptomatic and are usually
brought to a physician’s attention because of the Bowenoid papulosis. Slightly hyperpigmented
patient’s concern for genital warts. For undefined papules on the shaft of the penis
reasons, circumcision appears to help prevent penile
cancer. It has been theorized that the uncircumcised
male is at higher risk for penile carcinoma because of
retention of smegma and chronic maceration, which
can provide a portal for HPV infection, in conjunction
with chronic low-grade inflammation.
Pathogenesis: Almost all lesions of bowenoid papu-
losis have evidence of HPV. HPV subtype 16 is by far
the most predominant HPV type found in bowenoid
papulosis. Cells of the genital region that are chroni-
cally infected with HPV express various proteins that
are critical in the transformation into cancer. The best-
studied HPV oncoproteins, the E6 and E7 proteins,
can disrupt normal cell signaling in the p16 (TP16)
and retinoblastoma (RB) pathways. This disruption can
lead to a loss of control of cell signaling and loss of
normal apoptosis. These alterations eventually result in with visible mitoses. Evidence of HPV infection is transmission to the patient’s sexual partners must be
loss of the normal cell processes and the development almost universally seen as cells mimicking vacuolated addressed. Condoms should be used at all times to
of cancer. koilocyte cells. Special techniques such as polymerase help decrease the risk of transmission. Topical therapy
Histology: The histology is almost the same as that chain reaction (PCR) can be used to look for HPV with 5-fluorouracil or imiquimod has been advocated
of SCC in situ. There is full-thickness atypia of the subtyping. as the first-line therapy. Surgical treatment with
epidermis with involvement of the adnexal structures Treatment: After biopsy has ruled out an invasive electrocautery, cryotherapy, or laser ablation has also
and a well-intact basement membrane zone. Varying component to this tumor, the main treatment of been reported to be successful. Both patients and their
amounts of epidermal acanthosis and hyperkeratosis are bowenoid papulosis is to clinically remove the areas sexual partners should be seen for routine follow-up
seen. The cells are often enlarged and pleomorphic of involvement. The importance of decreasing HPV examinations.
THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS 57